Download
1 / 53
660 likes | 1.24k Views
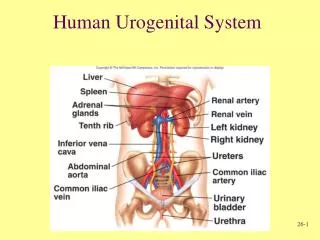
DEVELOPMENT OF UROGENITAL SYSTEM. DEVELOPMENT OF UREGENITAL SYSTEM. The urinary and reproductive systems a closely linked both in terms of their adult anatomy and embryological development. In all vertebrates the kidneys and ureters develop out of the intermediate mesoderm ,

E N D
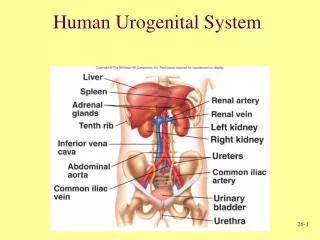
DEVELOPMENT OF UREGENITAL SYSTEM • The urinary and reproductive systems a closely linked both in terms of their adult anatomy and embryological development. • In all vertebrates the kidneys and ureters develop out of the intermediate mesoderm, • Whereas bladder and urethra derive from the urogenital sinus.
DEVELOPMENT OF UREGENITAL SYSTEM • The development of the urinary system is closely related to that of the genital system. • The urinary organs consist of the kidneys (which produce urine, among other things), the ureter (transport of the urine from the kidneys to the bladder), the bladder (temporary storage for the urine) and the urethra (transport of the urine from the bladder to the external world). • The urinary system begins to develop first and is semi-functional before the genital system appears.
DEVELOPMENT OF URINARY TRACT • All the nephrons we will ever have are in our kidneys at birth. • Most the Urinary tract system growth will occur by 5 years of age and with completed growth in adolescence. • Kidney function is immature during the first 2 years of life and is less efficient at fluid and electrolyte balance and drug elimination. • Poor concentration of urine increases urinary output per kg of body weight in infants than in childhood or adolescence. • Bladder capacity increases with age from 20 to 50 ml at birth to 700 ml as an adult • Children less than age 2 can not maintain bladder control because of insufficient nerve development
DEVELOPMENT OF URINARY TRACT • The kidney develops from the intermediate column of mesoderm. • There are actually three phases: • Earliest, are the pronephros, primitive tubules that develop in the cervical region and are vestigial (rudimentary) in us. • Next are the mesonephros (middle kidney) which consists of a duct that runs the length of the embryo, opening into the cloaca, and the nephric tubules. • The true, hind kidneys (called metanephros) develop in the sacral region. • The first two developmental stages have a transitory character and the definitive kidneys actually develop from the metanephros stage
EARLY DEVELOPMENT OF URINARY TRACT • Paraxial mesoderm • Intermediate mesoderm • Lateral mesoderm • Notochord • Amnion • Intraembryonic coelom • Endoderm • Ectoderm • Somatopleural (mesoderm and ectoderm) • Splanchnopleural (mesoderm and endoderm) • Neural groove • Neural ridge • Due to the lateral folding, the intermediate mesoderm is shifted ventrally and loses its connection with the somites and the lateral mesoderm. • The nephrogenic cord develops out of the intermediate mesoderm and extends from the cervical to the caudal region. Figure: Transverse section (in the midcephalic region) with a dorsal view of the three-layered embryo towards the end of the 3rd week of development. The intermediate mesoderm lies between the somites (paraxial mesoderm) and the lateral mesoderm (out of which the coelom arises).
EARLY DEVELOPMENT OF URINARY TRACT • Neural tube • Amniotic cavity • Paraxial mesoderm • Intermediate mesoderm • Yolk sac (umbilical vesicle) • It becomes segmented like the paraxial mesoderm (somites). • This segmentation is easily seen in the cranial region, and is rudimentary in the middle region. • In the caudal region it is no longer present. Figure: Transverse section of an embryo at the beginning of the folding (ca. 28 days; Stage 10). In this diagram the nephrogenic cord is clearly distinguished in the intermediate mesoderm. The black arrow indicates the border between the paraxial and intermediate mesoderm.
EARLY DEVELOPMENT OF URINARY TRACT • Neural tube • Amniotic cavity • Dermatomyome (somites) • Nephrogenic cord that has moved away from the paraxial mesoderm (somite) (black arrow) • Yolk sac (umbilical vesicle) • Notochord • Aorta • Intraembryonic coelom • Due to the growth of the inner structures of the embryo, the tissue lying most laterally is displaced ventrally. • This leads not only to a separation of the nephrogenic cord from the paraxial and lateral mesoderm, but also to a coalescence (blend) of certain median structures such as the two dorsal aortas which fuse to form the definitive (median) aorta. Stage 11 Stage 12 Figure: The intermediate mesoderm moves ventrally and loses its connection (black arrow) to the somites and the lateral mesoderm. Also observe its approach towards the intraembryonic coelom.
PRONEPHROS (FOREKIDNEY) DEVELOPMENT • The pronephros develops during the 4th week, beginning in the cranial part of the nephrogenic cord • And it atrophies during the 5th week. • Three characteristic pronephros structures can be distinguished: • The pronephros duct (Carnegie Stage 10) in the neck region • The pronephros tubules(Carnegie Stage 11) • The external or coelom glomeruli(Carnegie Stage 13) that have been shown to exist in humans.
PRONEPHROS (FOREKIDNEY) DEVELOPMENT • In humans, this pronephros system corresponds more to a primitive and transient structure that is functionally of no importance. • According to the classical view, the pronephros duct stops in the caudal region at the level of the 13th -14th somite and then goes over into the mesonephric duct (Wolffian duct). • Nephrogenic cord • Mesonephric duct (Wolff) • 1+2: Mesonephros • Intestinal tube • Cloaca • Atrophying nephrotomes • Yolk sac (umbilical vesicle) • Allantois • Outflow of the mesonephric duct into the cloaca
MESONEPHROS DEVELOPMENT • The mesonephros differentiates itself during the 4th week and after the 8th week it degenerates. • It replaces the pronephros and develops from three structures: • Nephrogenic cord(Carnegie Stage 10) in the dorso-lumbal region • Mesonephric duct(Carnegie Stage 11). • Glomerular capillary network(Carnegie Stage 13). • The mesonephric duct forms on the dorsal side of the nephrogenic cord at the level of the 9th somite. • Initially it consists of a solid mesenchymal cord of cells(Carnegie Stage 11). • Nephrogenic cord • Mesonephric duct • 1+2 Mesonephros • Intestine • Cloaca • Atrophied nephrotome • Yolk sac (umbilical vesicle) • Allantois • Outflow of the mesonephric duct into the cloaca • Ureter bud (anlage) Figure: Sagittal section of a 5-week-old embryo. The pronephros atrophies while the mesonephric duct grows caudally and fuses with the cloaca wall. In this stage, it goes through a mesenchymal- epithelial transformation and forms a central lumen. Only the caudal part remains mesenchymal. Observe the ureter bud at its caudal end.
MESONEPHROS DEVELOPMENT • It releases itself from the nephrogenic cord and is finally localized under the ectoderm, which probably plays an inductive role in its formation. • Released from the nephrogenic cord, it develops in the caudal direction and canalizes itself at the same time (Carnegie Stage 12), in order to finally end in the cloaca. • As soon as it is canalized one calls it the mesonephric duct (Wolffian duct). • At the site where the mesonephric duct (Wolffian duct) discharges into the cloaca, the rear wall of the bladder forms. Figure: The urogenital ridge projects into the lumen of the coelom. With the S-shaped mesonephric tubules the mesonephric duct (Wolffian duct) forms a transitory precursor of the adult excretory system. The medial end of the mesonephric tubule is closed and forms a funnel (Bowman’s capsule) that surrounds a tuft of capillaries (the glomerulus). The capillaries come from lateral branches of the dorsal aorta and drain into the inferior cardinal vein. This functional unit is also termed the excretory unit of the mesonephros. • LEGEND. • Neural tube • Notochord • Aorta dorsalis • Dorsal mesentery • Intestinal tube • Ectoderm • Somite • Inferior cardinal vein • Mesonephric duct (Wolffian duct) • Mesonephric tubule • Urogenital ridge
MESONEPHROS DEVELOPMENT • CS: 11; Day 29 • Arching of the intermediate mesoderm and forms from the nephrogenic chord. • Begining to differantiation in the caudal region • LEGEND • Inferior Cardinal Vein • Aorta dorsalis • Nephrogenic chord • Mesonephric duct (Wolffian duct) • Mesonephric vesicle • Subcardinal vein • Genital ridge • Dorsal mesentery • Intestinal tube
MESONEPHROS DEVELOPMENT • During stage 12; Day 30. • First polarized epithelial cells form out of the initially mesodermal condensate and differentiate themselves into mesonephros vesicle. • They bind with the mesonephric duct. • LEGEND • Inferior Cardinal Vein • Aorta dorsalis • Nephrogenic chord • Mesonephric duct (Wolffian duct) • Mesonephric vesicle • Subcardinal vein • Genital ridge • Dorsal mesentery • Intestinal tube • Mesonephric tubule
MESONEPHROS DEVELOPMENT • During stage 13; Day 32. • These vesicles differentiate themselves to become mesonephric tubules and take up a connection with the mesonephric duct. • Thus the first excretory unit are engendered that are very similar to the nephrons in the adult • LEGEND • Inferior Cardinal Vein • Aorta dorsalis • Nephrogenic chord • Mesonephric duct (Wolffian duct) • Mesonephric vesicle • Subcardinal vein • Genital ridge • Dorsal mesentery • Intestinal tube • Mesonephric tubule • Lateral branch of aorta
MESONEPHROS DEVELOPMENT • During stage 15; Day 36. • The tubule ends, which terminate medially, form themselves into a funnel that envelops a tuft of capillaries (Glomerulus). • This stem from arterial branch of the dorsal aorta. • LEGEND • Inferior Cardinal Vein • Aorta dorsalis • Nephrogenic chord • Mesonephric duct (Wolffian duct) • Mesonephric vesicle • Subcardinal vein • Genital ridge • Dorsal mesentery • Intestinal tube • Mesonephric tubule • Lateral branch of aorta • Glomerulus • Bowman capsule
MESONEPHROS DEVELOPMENT • During stage 17; Day 41. • These excretory mesonephric units begin to function and from the 6th week they start to produce urine. • After 10 weeks, they cease their function again and atrophy. • LEGEND • Inferior Cardinal Vein • Aorta dorsalis • Nephrogenic chord • Mesonephric duct (Wolffian duct) • Mesonephric vesicle • Subcardinal vein • Genital ridge • Dorsal mesentery • Intestinal tube • Mesonephric tubule • Lateral branch of aorta • Glomerulus • Bowman capsule
METANEPHROS: DEFINITIVE KIDNEY • The metanephros develops from three intermediate mesoderm structures of the sacral region: • Ureter anlage (Primordium, Bud)(CS 14 ) • Metanephric vesicle CS 13) • Glomerular capillary network (CS 13) • The ureter anlage is an epithelial diverticulum from the caudal part of the mesonephric duct (Wolffian duct) in the area of the first sacral vertebra (S1). • The primordium intrudes into the metanephric vesicle and forms the extra- and intrarenal excretory passages. • LEGEND • 1a. Pronephros (atrophying) • 1b. Mesonephros (atrophying) • Mesonephric duct (Wolffian duct) • Nephrogenic cord • Ureter anlage • Metanephric blastema • Liver anlage • Cloaca
METANEPHROS: DEFINITIVE KIDNEY • It is mesenchymal tissue out of which the metanephric vesicles arise. • From these originate the nephrons (= functional units of the kidneys). • At present it is still not clear whether the glomerular capillary network develops through vasculogenesis (direct development of vessels from the metanephric vesicles) or through angiogenesis (development from existing vessels of the metanephros). • LEGEND • 1a. Pronephros (atrophying) • 1b. Mesonephros (atrophying) • Mesonephric duct (Wolffian duct) • Nephrogenic cord • Ureter anlage • Metanephric blastema • Liver anlage • Cloaca
URETER ANLAGE (PRIMORDIUM) AND METANEPHRIC BLASTEMA • The interaction between the ureter anlage (epithelial tissue) and the metanephric blastema (mesenchyma) is of decisive importance for renal development. • The development of the kidneys represents a classical model of a sequential and reciprocal induction between epithelium and mesenchyma. • Renal development comprises a whole series of developmental processes such as forming an epithelial tree structure, interactive tissue induction, differentiation, polarization, migration, cell adhesion and finally the epithelio-mesenchymal transformation. • During the genesis of the metanephros the metanephric blastema first induces the branching of the ureter anlage, which, for its part, then lets the metanephric vesicle form into a predetermined blastema. • Through the transformation into epithelial tissue, the renal tubules form and finally the nephrons emerge.
RENAL EXCRETORY SYSTEM • The ureter anlage (bud, primordium) is an epithelial diverticulum which arises from the caudal portion of the mesonephric duct (Wolffian duct) at the level of the first sacral vertebra. • Its enlarged end grows in the dorso-cranial direction and projects into the metanephric blastema. • It is the origin of the intra- and extrarenal excretory passages: • Ureter • Renal pelvis • Major and minor calices • Collecting ducts • LEGEND: • Ureter • Major calix • Minor calix • Renal pelvis • Collecting duct • Metanephric vesicle • Kidney lobe
RENAL EXCRETORY SYSTEM • The renal pelvis arises from the swollen end of the ureteric bud (CS 16) that subdivides 4 times over the course of the 4th to 6th weeks. • 16 branches arise from this that partially then coalesce again in order to finally form 2 to 4 major calices. • At around the 7th week the minor calices start to develop. • They discharge into the major calices. • Further dichotomic branching follow - up to the 15th generation (roughly 32 weeks). • Thereby the caliber of the tubules is reduced more and more so that finally 1-3 millions collecting ducts are formed in the periphery of the metanephric blastema. • LEGEND: • 3. Minor calix • 5. Collecting duct • Distal tubule • Proximal tubule • Glomerulus • Connecting tubule • Intermediate tubule
RENAL EXCRETORY SYSTEM • During Stage 14; Day 33. • The Ureteric bud develops from caudal part of the mesonephric duct and grows in the dorso-cranial direction into the mesonephric blastema. • It subdivides dichotomically into 2, then 4 branches. • From its originally enlarged ends arises the renal pelvis, the stem forms the ureter. • LEGEND: • Ureter • Metanephric blastema • 1st dichotomous partition (two branches) • 2nd dichotomous partition (4 branches)
RENAL EXCRETORY SYSTEM • During Stage 16-17; Day 39-41. • 8 branches arises the third dichotomic from the original ureter primordium. • LEGEND: • 1st dichotomous partition (two branches) • 2nd dichotomous partition (4 branches) • 3rd dichotomous partition (8 branches)
RENAL EXCRETORY SYSTEM • During Stage 18; Day 44. • The original enlargement divides itself four times and 16 branches are so produced. • These merge again and form the 2-4 major calices, which finally form the continuation of the renal pelvis. • LEGEND: • 1st dichotomous partition (two branches) • 2nd dichotomous partition (4 branches) • 3rd dichotomous partition (8 branches) • 4th dichotomous partition (16 branches)
RENAL EXCRETORY SYSTEM • During Stage18-20; Day 44-46. • The following four division atrophy again and form themselves thereby into the minor calices. • The collecting ducts, which also divide in dichotomic way, drain the minor calices. • LEGEND: • Ureter • Minor calix • Major calix • Renal pelvis • Collecting duct • 1st dichotomous partition (two branches) • 2nd dichotomous partition (4 branches) • 3rd dichotomous partition (8 branches) • 4th dichotomous partition (16 branches) • Atrophy of the previous partitions (16 branches)
RENAL EXCRETORY SYSTEM • During Stage 18; Day 44. • The 5th generation and higher differentiate themselves from the tubules of the definitive collecting duct. • In the 32nd week the collecting duct have divided up to the 15th generation. • LEGEND: • Minor calix • Collecting duct • Papillary duct
METANEPHRIC BLASTEMA AND THE FORMATION OF THE NEPHRON • The process of nephron formation is complicated and thus subdivided into various steps: • The metanephric blastema surrounds each newly formed collecting duct. • It condenses in order to form peritubular cell aggregates. • Through induction signals, derived from the ureter primordium, the mesenchymal cells transform themselves and form vesicles.
THE FORMATION OF THE NEPHRON • During Stage 13, Day 32; • Each collecting duct is surrounded by metanephrogenic blastema. • It become condensed and forms dense peritubular cell aggregates that via gen activation. • Differentiate themselves to become Nephrons • LEGEND: • Collecting duct • 1a. Collecting duct lumen • Concentration of the metanephric blastema into cell aggregates • Neighboring metanephric tissue
THE FORMATION OF THE NEPHRON • During Stage 19, Day 46; • Due to the diffusible signal substances (WT-1, HNF-1 etc.)of the ureteic bud, the mesenchymal cell transform into epithelial tissue and form vesicles. • LEGEND: • Collecting duct • 1a. Collecting duct lumen • Concentration of the metanephric blastema into cell aggregates • Neighboring metanephric tissue
METANEPHRIC BLASTEMA AND THE FORMATION OF THE NEPHRON • During Stage 20, Day 47; • These vesicles lengthen and form S- shaped tubule that exhibit 3 section. • Legend: • Collecting duct • 1a. Collecting duct lumen • Metanephric vesicle (cut section) • Newly-created dichotomous division • New branch of the collecting duct
METANEPHRIC BLASTEMA AND THE FORMATION OF THE NEPHRON • During Stage 20, Day 49; • The epithelium, which comes into contact with an afferent arteriole, becomes thinner and forms a funnel with a double layered structure; Bowman Capsule. • Legend: • Collecting duct • New branch of the collecting duct • Metanephric vesicle that forms a tubule • Bowman's capsule • Afferent arteriole
METANEPHRIC BLASTEMA AND THE FORMATION OF THE NEPHRON • During Stage 21, Day 50; • At the same time in which the renal corpuscle forms, the other end of the original vesicle joins up with the distal parts of the collecting duct. • LEGEND: • Collecting duct • Metanephric vesicle that forms a tubule • Bowman's capsule • Afferent arteriole
METANEPHRIC BLASTEMA AND THE FORMATION OF THE NEPHRON • During Stage 21-end, Day 51; • The development of tubular system has progressed so far that the glomerular capsule forms from the proximal segment (and with the glomerulus forms a functional renal corpuscle). • Legend: • Collecting duct • Bowman's capsule • Afferent arteriole • Proximal convoluted tubule • Distal convoluted tubule • Proximal straight tubule • Distal straight tubule
METANEPHRIC BLASTEMA AND THE FORMATION OF THE NEPHRON • During Stage 23,Day 56; • The development of the tubuler system completed. • The distal segments forms the distal tubule and ascending thin limb of the intermediate tubule (Henle). • The middle segment forms the proximal tubule and the descending thin limb of the intermediate tubule (Henle). • LEGEND: • Collecting duct • Bowman's capsule • Afferent arteriole • Proximal convoluted tubule • Distal convoluted tubule • Proximal straight tubule • Distal straight tubule
METANEPHRIC BLASTEMA AND THE FORMATION OF THE NEPHRON • The epithelial vesicle secretes angiogenic factors. • Thereby, over the course of the further development, endothelial cells are brought into the glomerular capsule. • As soon as the afferent vessels come into close contact with the vesicular epithelium, it flattens and forms a cup with a bilaminar structure;Bowman's capsule. • At the same time as the formation of the renal corpuscle, the distal end of the epithelial vesicle fuses with the neighboring collecting duct. • LEGEND: • Collecting duct • Bowman's capsule • Afferent arteriole • Proximal convoluted tubule • Distal convoluted tubule • Proximal straight tubule • Distal straight tubule
ASCENT OF THE KIDNEY • The metanephros is formed in the sacral region at the level of the first sacral vertebra (S1) and the bifurcation of the aorta. • In the adult, the kidney lies at the upper lumbar level. • The "migration" (ascent) of the kidney occurs between the 6th and 9th week and the kidneys finally come to lie at the level of the 12th thoracal vertebra (Th12) under the suprarenal glands. • Legend: • Gonad • Mesonephros • Allantois • Tuberculum genitale • Cloacal membrane • Cloaca • 6a. Rectum • Posterior intestine • Metanephros • Mesonephric duct (Wolffian duct) • Ureter anlage
ASCENT OF THE KIDNEY • The mechanism that leads to this ascent of the kidneys is not an active migration but rather much more the result of the differing growths of the sacral and lumbar regions, which lead to an unfolding of the lower pole of the embryonic body. • During its ascent, the kidney is supplied by a number of transitory vessels that all originate from the aorta. • The definitive renal arteries stem from the lumbar region of the aorta, while the transitory vessels normally disappear. • Legend: • Gonad • Mesonephros • Allantois • Tuberculum genitale • Cloacal membrane • Cloaca • 6a. Rectum • Posterior intestine • Metanephros • Mesonephric duct (Wolffian duct) • Ureter anlage • 10a. Ureter • Urogenital orifice • Anal orifice
ASCENT OF THE KIDNEY • It must also be mentioned here that during their development the kidneys turn 90° towards the vertebral cords, so that the hili are medially oriented at the end, while they originally face ventrally. • Various anomalies are connected with this ascent • Legend: • Gonad • Mesonephros • Allantois • Tuberculum genitale • Cloacal membrane • Cloaca • 6a. Rectum • Posterior intestine • Metanephros • Mesonephric duct (Wolffian duct) • Ureter anlage • 10a. Ureter • Urogenital orifice • Anal orifice
FUNCTIONAL DEVELOPMENT OF THE KIDNEY • The metanephros thus becomes able to function and can filter the plasma from the glomeruli. • Through the proximal tubule the glomerular filtrate (primary urine) gets into the intermediate tubule, the distal tubule, connecting tubules and collecting duct. • In these tubules the secondary urine arises through resorption and secretion processes. • It then reaches the renal pelvis and, via the ureter, the bladder. • During the pregnancy, the fetal urine is excreted into the amniotic cavity.
FUNCTIONAL DEVELOPMENT OF THE KIDNEY • At birth the kidneys have a multilobular appearance, due to the development of the ureteric bud in the metanephric blastema. • Normally, towards the end of the fetal period, the lobes are considerablysmoothed, but they still exist until after birth. • Completion of the smoothing follows during childhood by the increase in volume of the connective tissue and the increase in size of the nephrons without any change in their number. • With only few exceptions, adult kidneys no longer exhibit any lobulation. • Since the renal architecture is finalized between the 5th and 15th weeks of intrauterine development; organogenesis of the kidneys lasts well beyond the embryonic phase until far into thefetal period.
LEGEND: • Medullary rays • Papilla renalis • Sinus renalis • Columna renalis • Medullary pyramid • Interlobar artery • Interlobar vein • Arcuate artery • Arcuate vein • Interlobular arteries and veins
RENAL AGENESIS AND DYSPLASIA • Kidneys may fail to develop on one or both sides due to faulty tissue-tissue interactions between the ureteric bud and nephrogenic and stromalmesenchyme. • Infants with bilateral renal agenesis are stillborn or die within a few days of birth. • In contrast, infants with unilateral renal agenesis usually live because the remaining kidney undergoes compensatory hypertrophy. • Although the relative frequencies of unilateral and bilateral renal agenesis are difficult to determine because unilateral renal agenesis often goes undetected, autopsy data suggest that unilateral renal agenesis is about four to eight times more common than bilateral renal agenesis. • Renal agenesis is typically associated with other congenital defects. • The kidneys contribute to the production of amniotic fluid. • Therefore, bilateral renal agenesis results in oligohydramnios, or insufficient amniotic fluid. • Oligohydramnioscan result in a spectrum of abnormalities called Potter sequence. • These include deformed limbs; wrinkly, dry skin; and an abnormal facies (in this context, facies means "facial appearance") consisting of wide-set eyes with infraorbital skin creases, beak nose, recessed chin, and low-set ears.
RENAL AGENESIS • Renal agenesis is often associated with a spectrum of ipsilateral genitourinary abnormalities, including defects in structures derived from the mesonephric duct in males and Müllerian duct in females. • Failure of mesonephric duct development leads to absence of both the vas deferens and kidney, because the kidney develops from an outgrowth of this duct, which in the male is the progenitor of the vas deferens. • This can occur bilaterally or unilaterally.
RENAL DYSPLASIA • Abnormal kidneys may arise from abnormal inductive interactions. • In some cases, subtle defects in the interaction between ureteric bud and metanephricblastema result in hypoplasia or dysplasia of the developing kidney. • The small number of nephrons in a hypoplastic kidney results either from inadequate branching of the ureteric bud or from an inadequate response by the metanephric cap tissue. • In cases of renal dysplasia, the nephrons themselves develop abnormally and consist of primitive ducts lined by undifferentiated epithelium sheathed within thick layers of connective tissue. • The genetic causes for some of these renal anomalies are beginning to be identified. • Mutations in PAX2 are associated with dominant transmission of renal hypoplasia and dysplasia (seen inrenal-coloboma syndrome). • Mutations in EYA1 (a transcription factor required for GDNF expression and, hence, ureteric bud development) and SIX1 (SINE OCULIS HOMEOBOX HOMOLOG 1; a transcription factor that interacts withEYA1) causes BOR (branchio-oto-renal) syndrome. • In addition to renal anomalies, EYA1 haploinsufficient individuals also develop pharyngeal cleft cysts and have both outer and inner ear defects.
CONGENITAL POLYCYSTIC KIDNEY DISEASE • Autosomal dominant polycystic kidney disease (ADPKD) is a common genetic disease associated with formation of cysts in the kidneys as well as in ductal epithelia in the liver, pancreas, testis, and ovary. • Mutations in the genes encoding POLYCYSTIN1 (PDK1) and POLYCYSTIN2 (PDK2) account for 85% and 15% of ADPKD, respectively. The precise roles of the POLYCYSTIN1 andPOLYCYSTIN2 proteins have not yet been elucidated. • However, POLYCYSTIN1seems to be required for normal elongation and maturation of tubular structures during renal development. • It may also function as a mechanosensory channel in primary cilia. • These functions may be related to PDK1's ability to modulate Wntsignaling by stabilizing endogenous β-Catenin levels and altering β-Catenin/ Tcf-dependent gene expression.