Download
1 / 19
220 likes | 497 Views
Neuroendocrine Tumours. Neuroendocrine Tumours. Heterogenous group of neoplasms Share certain characteristic features Originate from neuroendocrine cells Have secretory characteristics Frequently present with hypersectretory syndromes. Neuroendocrine Tumours. Pancreatic islet cells

E N D
Neuroendocrine Tumours • Heterogenous group of neoplasms • Share certain characteristic features • Originate from neuroendocrine cells • Have secretory characteristics • Frequently present with hypersectretory syndromes
Neuroendocrine Tumours Pancreatic islet cells Gastroenteric tissue Respiratory epithelium Gastroenteropancreatic NETs Includes carcinoid (serotonin secreting tumour)
Presentation • Asymptomatic • Present with obstructive symptoms • Symptoms • Usually due to liver metastases • Release of hormones into circulation e.g. Serotonin, tachykinin
Symptoms Intermittent abdo pain 70% Diarrhoea 50% Flushing 30% Lacrimation Rhinorrhoea Episodic palpitations Wheezing Pellagra
“Carcinoid crisis” Precipitated by Anaesthetic induction Intraoperative tumour handling Therapeutic procedures, eg embolisation Profound flushing Bronchospasm Tachycardia Widely fluctuating BP
Aetiology and Genetics Poorly understood Most are sporadic Small increased familial risk for small intestinal / colonic tumours Aim to exclude complex cancer syndromes (e.g. MEN 1, MEN 2, NF1)
Diagnosis Clinical symptoms Hormone concentrations Radiology Histology – gold standard
Hormone concentrations • Plasma chromagranin A (CgA) • May correlate with response and relapse • Fast rising levels = poor prognosis • Urine 5-HIAA (24 hrs) • Certain foods affect urinary excretion and may cause false positives • Pancreatic polypeptide • High concentration in 80% pancreatic and 50% carcinoid • Should also measure other hormones for MEN syndromes.
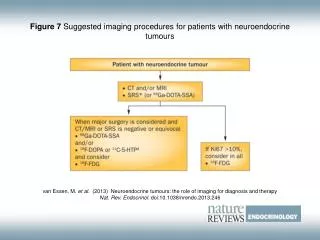
ImagingSensitivites (%) of various imaging modalities for locating specific neuroendocrine tumours
Imaging 40-70% of patients have nodal or liver metastases at time of presentation If <2 cm diameter: low incidence of metastases
Small intestinal carcinoid: Treatment • Aim should be curative • Palliation in majority of cases • Majority are malignant • Resection of primary and mesenteric lymph nodes despite liver mets • For cure / delay progression (could endanger small bowel) • Can alleviate symptoms • ? Prolong survival
Symptomatic Treatment • Used in patient with secretory symptoms • Somatostatin analogues (e.g. Octreotide) • Inhibits release of many hormones • Can impair some exocrine functions • Hormone response in 30-70% patients • Symptom control in majority • Rarely tumour shrinkage
Additional medication • Ondansatron • nausea • Cyproheptadine • Cholestyramine • CREON • Control of diarrhoea, esp after intestinal resection
Interferon alpha Sole use or with somatostatin analogues ? Efficacy (conflicting evidence) Some evidence better in tumour with low mitotic rates Biochemical response 40-60% Symptomatic improvement 40-70% Significant tumour shrinkage 10-15%
Other options • Chemotherapy • Role uncertain but being actively researched • Response short lived (8-10 months) • Hepatic artery embolisation • Indicated for non resectable & multiple hormone secreting tumours • Causes ischaemia of tumour cells • Symptomatic response 40-80% • 5 year survival 50-60%
Radionucleotide therapy • Palliative option • Exploits increased uptake of radiolabelled isotopes I-MIBG or octreotide • Symptom control 80% • Radiotherapy • Carcinoid – radioresistant • Relief of pain from bone mets
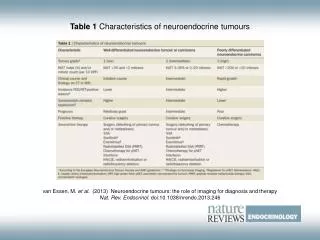
Prognosis • No TNM classification • Slow growing, but survival depends on • Histological type • Degree of differentiation • Mitotic rate • Tumour size • Depth and location • Lymph node/ liver metastases