Download
1 / 1
10 likes | 138 Views
AGE- AND GENDER-CORRECTED BODY MASS INDEX: A NEW APPROACH FOR MORTALITY RISK ASSESMENT IN ESOPHAGECTOMY FOR CANCER. J. Moons, H . Van Veer, W . Coosemans, T. Lerut, G . Decker, H. Decaluwe, D . Van Raemdonck, P. De Leyn, P . Nafteux

E N D
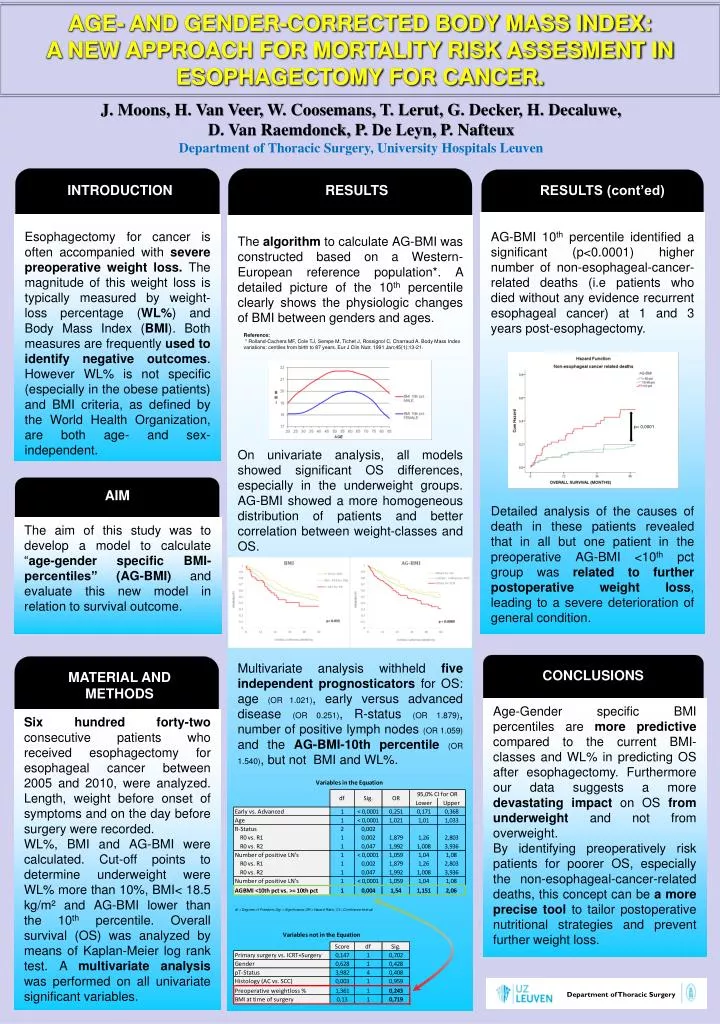
AGE- AND GENDER-CORRECTED BODY MASS INDEX: A NEW APPROACH FOR MORTALITY RISK ASSESMENT IN ESOPHAGECTOMY FOR CANCER. J. Moons, H. Van Veer, W. Coosemans, T. Lerut, G. Decker, H. Decaluwe, D. Van Raemdonck, P. De Leyn, P. Nafteux Department of ThoracicSurgery, University Hospitals Leuven INTRODUCTION RESULTS RESULTS (cont’ed) AG-BMI 10th percentile identified a significant (p<0.0001) higher number of non-esophageal-cancer- related deaths (i.e patients who died without any evidence recurrent esophageal cancer) at 1 and 3 years post-esophagectomy. Detailed analysis of the causes of death in these patients revealed that in all but one patient in the preoperative AG-BMI <10thpct group was related to further postoperative weight loss, leading to a severe deterioration of general condition. Esophagectomy for cancer is often accompanied with severe preoperative weight loss. The magnitude of this weight loss is typically measured by weight-loss percentage (WL%) and Body Mass Index (BMI). Both measures are frequently used to identify negative outcomes. However WL% is not specific (especially in the obese patients) and BMI criteria, as defined by the World Health Organization, are both age- and sex-independent. The algorithm to calculate AG-BMI was constructed based on a Western-European reference population*. A detailed picture of the 10th percentile clearly shows the physiologic changes of BMI between genders and ages. On univariate analysis, all models showed significant OS differences, especially in the underweight groups. AG-BMI showed a more homogeneous distribution of patients and better correlation between weight-classes and OS. Multivariate analysis withheld fiveindependent prognosticators for OS: age (OR 1.021), early versus advanced disease (OR 0.251), R-status (OR 1.879), number of positive lymph nodes (OR 1.059) and the AG-BMI-10th percentile(OR 1.540), but not BMI and WL%. Reference: * Rolland-Cachera MF, Cole TJ, Sempe M, Tichet J, Rossignol C, Charraud A. Body Mass Index variations: centilesfrombirthto 87 years. Eur J ClinNutr. 1991 Jan;45(1):13-21. p< 0,0001 AIM The aim of this study was to develop a model to calculate “age-gender specific BMI-percentiles” (AG-BMI) and evaluate this new model in relation to survival outcome. CONCLUSIONS MATERIAL AND METHODS Age-Gender specific BMI percentiles are more predictive compared to the current BMI-classes and WL% in predicting OS after esophagectomy. Furthermore our data suggests a more devastating impact on OS fromunderweight and not from overweight. By identifying preoperatively risk patients for poorer OS, especially the non-esophageal-cancer-related deaths, this concept can be a more precise tool to tailor postoperative nutritional strategies and prevent further weight loss. Six hundred forty-two consecutive patients who received esophagectomy for esophageal cancer between 2005 and 2010, were analyzed. Length, weight before onset of symptoms and on the day before surgery were recorded. WL%, BMI and AG-BMI were calculated. Cut-off points to determine underweight were WL% more than 10%, BMI< 18.5 kg/m² and AG-BMI lower than the 10th percentile. Overall survival (OS) was analyzed by means of Kaplan-Meier log rank test. A multivariate analysis was performed on all univariate significant variables. Department of Thoracic Surgery






