Download

1 / 31
340 likes | 604 Views
Newcastle Fertility Centre @. Potential of new reproductive technologies in reducing the risk of mitochondrial DNA disease . Mary Herbert PhD Professor of Reproductive Biology Newcastle University. Mitochondrial DNA ( mtDNA ) is maternally inherited. X. Day 1. Day 2. Day 3. Blastocyst

E N D
Newcastle Fertility Centre @ Potential of new reproductive technologies in reducing the risk of mitochondrial DNA disease Mary Herbert PhD Professor of Reproductive Biology Newcastle University
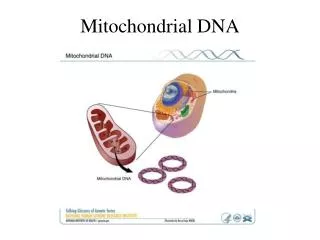
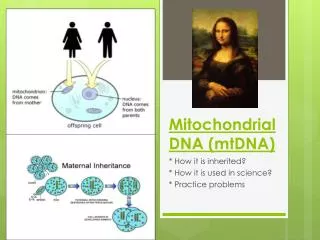
Mitochondrial DNA (mtDNA) is maternally inherited X Day 1 Day 2 Day 3 Blastocyst 64-200 cells Day 5-6
Women who carry a mix of normal and mutated mtDNA produce eggs with varying levels of mutation Mutation load
What are the currently available options for reducing risk of transmitting mtDNA mutations? • Egg Donation • Pre-implantation genetic diagnosis (PGD)
Pre-implantation genetic diagnosis (PGD) Well established technique for preventing transmission of defects in the nuclear genome • IVF treatment • Removal of one or two cells from 6-8 cell embryos • Genetic analysis
PGD for reducing risk of transmitting mtDNA disease Mutation load • 1-2 cells analysed to select embryos with lowest mutation load • Mutation load of biopsied cell representative of the entire embryo? Evidence so far indicates that this is not a problem • Not useful in cases where 100% of mtDNA is mutated
Are there alternative strategies for cases with high mutations loads? Can we uncouple the inheritance of nuclear DNA from mtDNA? Transplantation of the nuclear DNA? Mutation load
Nuclear genome transplantation: current options Transfer of meiotic spindle and associated chromosomes Unfertilised egg Fertilised egg Transfer of pronuclei
Pronuclear Transfer (PNT) Donor egg Egg from affected woman Meiosis II Spindle Transfer (MST) Donor egg Egg from affected woman wild-type mitochondria mutant mitochondria
Pronuclear transfer (PNT) • Proven to be compatible with development in mice (McGrath and Solter, 1983; Meirelles & Smith, 1997) • Proven to prevent transmission of a mtDNA deletion in mice (Sato et al, PNAS, 2005)
Pronuclear transfer in human zygotes • Is it technically feasible? • Can we minimise the level of mtDNA carryover? • Can reconstituted zygotes develop to the • blastocyst stage?
Research Material • No ready supply of normally fertilised zygotes available for research • Initial experiments performed on abnormally fertilised human zygotes (mono-pronucleate and tri-pronucleate)
Step 1 Removal of pronuclei Requires cytoskeletal Inhibitors to depolymerize the actin and microtubule networks Test for reversibility andcytotoxicity
Step 2 Fusion of karyoplast with enucleated zygote • Electrical fusion: problem with lysis of zygotes • - Inactivated Sendai viral envelope protein (HVJ-E)
Blastocyst development following PNT using abnormally fertilised zygotes Unmanipulated controls: 17% Pronuclear transfer: 8% < 2% mtDNA carryover Craven et al, 2010, Nature, vol. 465
Ongoing work: Testing Safety and Efficacy (in vitro studies) • Effect of pronuclear transfer on embryo development of normally fertilised eggs • Maximise the yield of high quality blastocysts • Test for normality using a range of parameters to compare PNT with control blastocysts • Fate of karyoplast-associated mtDNA? • In vitro studies to compare PNT and MST
Additional in vitro studies to test likely safety and efficacy or PNT and MST UK: Expert Panel convened by the Human Fertilisation and Embryology Authority (HFEA)
Minimum set of experiments required • MST in human oocytes that are then fertilised • PNT using normally fertilised human oocytes • Pronuclear transfer in a non-human primate model – demonstrate that offspring are normal
Additional in vitro studies to test likely efficacy: Analysis of blastocysts Yolk sac Primitive Endoderm Trophectoderm Placenta Inner Cell Mass Epiblast Embryonic stem cells Foetal Tissues The establishment of a viable pregnancy requires: Epiblast + Trophectoderm+ Primitive endoderm
Blastocyst morphology predictsclinical outcome Blastocyst morphology scoring - degree of expansion - size and compactness of the ICM - trophectoderm morphology Blastocyst quality: Grade A Grade B Grade C Clinical pregnancy: 60.3% (n=68) 32.7 (n=10) 0% (n=7) Blastocyst quality is important - Information on this is currently Iacking for PNT and MST
Summary: Additional in vitro studies • Further in vitro tests for efficacy and safety • To enable couples who might benefit from the new techniques to make an informed decision • Likely to lead to further refinements of the procedures • Increase the likelihood of success in a future clinical trial
Nuffield Council on Bioethics …on balance we believe that if these novel techniques are adequately proven to be acceptably safe and effective as treatments, it would be ethical for families to use them, if they wish to do so and have been offered an appropriate level of information and support. .
Future clinical studies (1) Enrolment/Indications • Initially offer only to women with high levels of pathogenic mtDNA mutations • - Balance of risk and benefit • Initial investigations should be confined to young (<35) women with a good ovarian reserve • - Avoid confounding effect of female reproductive ageing
Future clinical studies (2) Donors • Age (<35 years) with good ovarian reserve • Preferably with proven fertility • Test run to check embryo viability after oocyte vitrification • Match for mtDNAhaplotype
Future clinical studies (3) Follow-up • Follow-up during pregnancy • Detailed analysis in the event of spontaneous abortion • Long term follow up of any children born
MST for age-related infertility? Missegregation of chromosomes during meiosis is the major cause of infertility in older women (>70% of oocytes affected) Normal Abnormal
MST for age-related infertility? Abnormal Normal The segregation errors and/or structural defects that give rise to aneuploidy have already occurred by the time the MII oocyte is harvested from the ovary Difficult to envisage how MST (or PNT) could correct meiotic segregation errors
Clinical studies on the use of MST (or PNT) to treat age-related infertility are likely to produce misleading results regarding the safety of these procedures
Next steps to potential clinical treatment in the UK June 2013: Government announced decision to draft Regulations to amend the HFE Act to permit the clinical application of PNT and MST for preventing transmission of mtDNA disease • Publication and consultation of the Draft Regulations • Debate and votes in both Houses of Parliament on the final version of the Regulations • If passed, detailed regulations agreed and adopted by the HFEA Clinical application confined to mtDNA disease
Louise Hyslop Laura Irving DimitriosKalleas Jessica Richardson Randy Ballesteros Meija QiZhang Doug Turnbull Lyndsey Craven Newcastle Fertility Centre @ Egg Donation programme Alison Murdoch MeenaChoudhary Research Nurses Maria Nesbitt Linda Burgess