Download
1 / 30
740 likes | 2.55k Views
Liver Function Tests (LFTs). Prepared by Hamad ALAssaf a lassaf_h@yahoo.com. Routine Liver Function Tests (LFTs) . LFTs are blood tests used to diagnose & monitor disease or damage of the liver: 1- Serum Albumin 2- Blood Liver Enzymes: - Alanine amino transferase (ALT)

E N D
Liver Function Tests (LFTs) Prepared by Hamad ALAssaf alassaf_h@yahoo.com
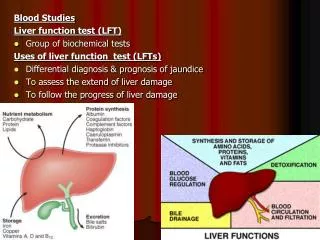
Routine Liver Function Tests (LFTs) LFTs are blood tests used to diagnose & monitor disease or damage of the liver: 1- Serum Albumin 2- Blood Liver Enzymes: - Alanine amino transferase (ALT) - Aspartate amino transferase (AST) - Gamma glutamyl transferase (GGT) - Alkaline phosphatase (ALP) 3- Blood Billirubin (total, direct & indirect) 4- Blood Coagulation Factors (prothrombin): Prothrombin Time (PT) 5- Markers of liver fibrosis
Serum Albumin • Albumin is present in higher concentrations than other plasma proteins ( ~ 40 g/L in normal adults). • Albumin is synthesized in the liver & has a half-life of 20 days. • Very small amounts of albumin cross the glomerular capillary wall. Accordingly, no more than traces of albumin may normally appear in urine that can not be detected by ordinary laboratory means. • Albuminuria: In this case, albumin can be detected in urine by ordinary laboratory means due to physiological or pathological conditions.
Serum Albumin • Causes of hypoalbuminemia: • Artifactual:Diluted sample • Physiological :Pregnancy • Decreased amino acids:Reduced essential amino acids in diet & reduced synthesis of nonessential amino acidsdue to either Malnutrition or Malabsorption. • Increased catabolism :Surgery, Trauma, Infections. • Defective synthesis in liver: Chronic liver diseases (liver cirrhosis) • Increased loss :From the kidney (Nephrotic syndrome)or From GIT (Protein loosing entropathies)
Blood Aminotransferases (ALT & AST) • Aminotransferases (ALT & AST) are normally intracellular enzymes. • Elevated blood levels of aminotransferases indicate damage to cells rich in these enzymes (as disease to tissue or physical trauma ) • Blood AST & ALT are of particular diagnostic value
Causes of elevated levels of blood ALT & AST • 1-Viral , toxic or alcholic hepatitis: • Highlyincrease in ALT & AST (Up to 20 - 50 folds). • In viral hepatitis, ALT is muchelevated than AST • 2- Cirrhosis (chronic liver diseases): • Moderateincrease (up to 4 – 5 folds) • In chronic cases, AST is muchelevated than ALT. • 3- Obstructive jaundice: • Moderateincrease ALT & AST are increased up to 3 folds. • 4- After alcoholic or drug intake: • Transientslight to moderate increase.
Alanine amino transferase (ALT) • ALT is moreliver specificthan AST. • ALTrarely increases in lesions other than the liver parenchymal • ALTelevations persist longerthan do AST. • Formerly namedas Glutamate pyruvate transferase (GPT) • Blood levels of ASTare increased with many diseases of various organs: • 1- Liver diseases • 2- Myocardial infarction (MI) • 3- Progressive skeletal muscular dystrophy • 4- Crush injury • 5- Hemolytic diseases • 6- Artifact: in hemolysed samples or if serum separation is delayed. • Formerly named as Glutamate oxaloacetate transferase (GOT) Aspartate transaminase (AST)
Gamma glutamyl transferase (GGT) • GGTpresent in blood originates primarily from hepatobiliary system • Causes of increased blood GGT: • 1- Induction of GGT synthesis by these cells occurs without cell damage • by alcohol or drugsas anticonvulsants. • 2- Biliary obstruction: • GGT is markedly increasedwith obstructive jaundice (5 – 30 folds) • Increase earlier (more sensitive) than ALP • Persists longerthan ALP • 3- Viral, toxic & alcoholic hepatitis : • Increase is only 2 – 5 folds (less sensitive than ALT & AST) • 4- Primary and secondary liver tumors: • GGT is elevated earlier than other enzymes in liver neoplasm. • Secondary of other organ tumors in the liver can be early detected by elevated GGT. (arouse suspicious that the diseases is metastatic to liver)
Alkaline Phosphatase (ALP) • Main Sources of ALP: • 1- Cells of hepatobiliary tract(hepatocytes adjacent to the biliary canalculi). • 2- Osteoblasts of bone : • 3- Other Sources: Intestine and placenta & renal tubules. • If ALP is elevated due to a bone disease • In this case, GGTis normal • i.e. GGTis used to ascertain whether increased ALPis due to boneor hepatobiliary disease
Alkaline Phosphatase (ALP) cont. • Clinical significance of increased serum ALP activities: • 1- Physiological increase of ALP: • During periods of active bone growth in infancyand at puberty. • Preterm infants total ALP is increased to 5 times the upper reference limit of adults due to bone isoenzymes. • In children under 3 years, total ALP activity is increased up to 2.5 times the upper limit. • Increased twice, during the second andthird trimesters of pregnancy (placental ALP).
Alkaline Phosphatase (ALP) cont. • 2- Pathological increase of ALP: • A-Bone causes: (due to increased osteoblastic activity): • Tumors (osteogenic) • Paget`s Disease of bone: Marked increase (10 – 25 folds) • Primary osteogenic tumors • Secondary malignant deposits in boneif causing osteoblastosis • Rickets & osteomalacia (vitamin D deficiency) • Primary & secondary hyperparathyroidism (increased PTH) • Healing of bone fractures
Alkaline Phosphatase (ALP) cont. • B- Hepatobiliray tract: liver diseases with involvement of biliary tract. • 1- Obstructive jaundice: • Extrahepatic cholestiasis : (Markedincrease, up to 10 – 12 folds) • Due to obstruction of to the flow of bile through the biliary tract e.g. Gallstones, cholecystitis. • Intrahepatic cholestiasis: (Moderate increase , ~ 3 -5 folds) • Bile secretion from the hepatocytes into the canalculi is impaired e.g. cholangitis. • 2- Viral, toxic & alcoholic hepatitis: • Mild to moderate increase, less than 3 folds.
Coagulation factors • The liver makes many of the proteins (clotting factors) needed to make blood clot. • In certain liver disorders the liver cannot make enough of these proteins and so blood does not clot so well. Therefore, blood clotting tests may be used as a marker of the severity of certain liver disorders • In liver disease, the synthesis of prothrombin & other clotting factors is diminished prolonged prothrombin Time (PT) • This may be one of the earliest abnormalities seen in hepatocellular damage, since prothrombin has a short half-life (~ 6 hours)
Markers of Liver Fibrosis • Procollagen type III terminal peptide • Hyaluronic acid (hyaluronin)
-Fetoprotein • One of the major plasma proteins in fetal life. • Falls thru-out gestation and by age one year • In acute hepatic injury AFP 10 – 20 folds. • Used to screen and diagnose Hepatocellular carcinoma & hepatoblastoma.
Ammonia • Ammoniais produced by all tissues from the catabolism of amino acids • Ammoniais mainly disposed is via formation of urea in liver • Blood level of ammoinamust be kept very low, otherwise, hyperammonemia& CNS toxicity will occur
catabolism of amino acids With production of Ammonia In Liver Small amount excreted in urine Urea
HyperammonemiaIncrease of ammonia level of blood • Normal level of blood ammonia is 5-50 mmol/L • Hyperammonemia : A medical emergency as ammonia has a direct neurotoxic effect on CNS • Ammonia intoxication: It is defined as toxicity of the brain due to increase in ammonia level in the systemic blood. • At high concentrations, ammonia can cause coma & death
Causes of Hyperammonemia 1- Liver diseases: are common causes in adults i- Acute causes: viral hepatitis, ischemia, hepatotoxins ii- Chronic causes: liver cirrhosis due to alcoholism, hepatitis, biliary obstruction. 2 - GatrointestinalBleeding: By action of bacteria of GIT on blood urea with production of much amounts of ammonia that is absorbed to blood. 3- Ornithine transcarbamoylasedeficiency (Hereditary)
Hyperammonemia in Renal Failure Renal Failure blood urea levels are elevated Transfer of urea to intestine is increased Much amounts of Ammonia is formed by bacterial urease Absorbed to blood Hyperammonemia
Precautions resampling, handling • A free‐flowing venous (or arterial) blood sample should be collected into a specimen tube (preferably pre‐chilled) containing either lithium heparin or EDTA • As difficult venepuncture can cause a spurious increase in [ammonia]. • The sample should be transported on iceto the laboratory, separated within 15 minutes of collection and analyzed immediately. • These precautions are necessary as the [ammonia] of standing blood increases spontaneously, due to generation and release of ammonia from red blood cells
Formation of Bilirubin from Heme Breakdown of RBCs Heme Biliverdin(green) Bilirubin(red-orange) bile pigments In Blood with albumin UNCONJUGATED BILIRUBIN (or INDIRECT BILITUBIN)
Bilirubin Metabolism in the Liver • Uptakeof Bilirubin by hepatocytes: Bilirubin dissociates from its carrier albumin & enters hepatocytes • Conjugation of Bilirubin: In hepatocytes, bilirubin is conjugated with two molecules of glucuronic acid by the enzyme glucuronyltransferase • Excretion of bilirubin into bile: Conjugated bilirubin (Direct bilirubin) is transported into bile canalculi & then into bile.
Bilirubin Metabolism in the Intestine Conjugated bilirubin bacteria in the intestine Urobilinogen Stercobilin Reabsorbed in stool (brown) Kidney Urine Urobilin(yellow)
Jaundice • Yellow color of skin, nail beds & sclera caused by deposition of bilirubin secondary to increased bilirubin levels in blood (hyperbilirubinemia)
Types of Jaundice 1- Hemolytic Jaundice: Massive lysis of RBCs in hemolytic anemia e.g. sickle cell anemia & G6PD deficiency anemia & Hemolytic transfusion reaction. 2- Obstructive Jaundice: Conjugated bilirubin is prevented from passing to the intestine. As in Gallstones. 3- Hepatocellular Jaundice: Liver damage (by hepatitis or cirrhosis) causes low conjugation efficiency leading to increased unconjugated (indirect) bilirubin in blood.
Jaundice in Newborns • In newborns (especially premature) Bilirubin accumulates as the liver enzyme bilirubin glucuronyltransferase (responsible for conjugation of bilirubin) is low at birth. (The enzymes reaches adult levels in about 4 weeks). • Accordingly, unconjugated bilirubin is increased in blood. • Elevated bilirubin in excess of the binding capacity of albumin can diffuse into basal ganglia & cause toxic encephalopathy (kernicterus) • Treatment • Exposure of the newborn skin to blue fluorescent light which converts bilirubin to more polar & hence water-soluble isomers • These isomers can be excreted into bile without conjugation to glucuronic acid.
Congenital hyperbilirubinemia Bilirubin is elevated in blood due to inherited defects in the bilirubin metabolic pathway 1- Crigler-Najjarsyndrome • Lowactivityof glucoronyltransferase (conjugating enzyme) • Severe hyperbilirubinemia in neonates (unconjugated bilirubin), Complicated by kernicterus & early death 2- Gilbert`s syndrome • Decreased production of glucoronyltransferase • More common in men, Occurs in 2-3 % of men. • Usually asymptomatic hyperbilirubinemiawith Normal Liver function tests. 3- Dubin-Johnson syndrome • Defect in transfer of conjugated bilirubin into the biliary canalculi Conjugated hyperbilirubinemia.