Download

1 / 23
250 likes | 577 Views
Motor and sensory deficits post stroke Judith Croxon-Stroud Clinical specialist physiotherapist May 2011. Objectives. To understand the motor and sensory deficits caused by stroke To be familiar with how the deficits are assessed To understand the effects these deficits have on function.

E N D
Motor and sensory deficits post stroke Judith Croxon-Stroud Clinical specialist physiotherapist May 2011
Objectives • To understand the motor and sensory deficits caused by stroke • To be familiar with how the deficits are assessed • To understand the effects these deficits have on function
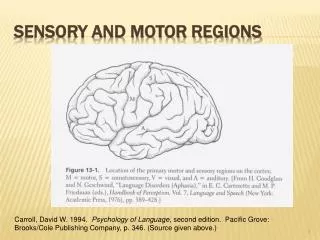
Frontal Lobe • Consciousness • Initiation • Judgement / reasoning • Emotional responses • Expressive language • Word associations • Abstract thinking • Memory for habits and motor activities
Lesions in Frontal Lobe • Mood changes • Dysexecutive syndrome – problem solving, organisation, sequencing and planning skills • Paralysis / hemiplegia • Rigidity of thought • Personality change and social behaviour • Perseveration • Inability to express language • Reduced insight • Incontinence
Parietal Lobe • Visual attention • Sensory awareness • Voluntary movement • Manipulation of objects
Lesions in Parietal Lobe • Only 1 task at a time • Spatial deficits • Anomia – unable to name objects • Agraphia – unable to write • Reading, math, drawing • Distinguishing right from left • Apraxia • Reduced visual attention • Reduced eye-hand co-ordination
Occipital lobe • Vision – interprets and discriminates visual stimuli Problems • Visual deficits • Hallucinations • Word blindness • Reduced reading and writing • Visual object agnosia
Temporal lobe • Understanding (interpreting language) • Formation of emotion • Hearing, memory, visual perception
Lesions in Temporal Lobe • Receptive dysphasia • Amnesia • Mood swings, change in sexual behaviour • Reduced face recognition • Selective attention problems • Reduced short term memory
Motor Deficits • Tone • Muscle weakness • Co-ordination
Sensory deficits • Light touch • Pin prick • Hot / cold • 2 point discrimination • Sensory extinction • Stereognosis
Tone • A state of variable activity and /or readiness within muscle • Adaptable to sensory / proprioceptive controls • Important for the maintenance of an upright posture • Adapt to a varying and changing base of support • Allows selective movement to attain functional skills
Muscle weakness - grading • Muscle strength important for all functional activities • Graded by assessing the strength of muscles using the Oxford Scale • Graded from 0 – 5 • Judged on what is normal taking in account of the persons age and sex • Knowledge of anatomy of muscle and joints is vital to allow accurate positioning of the joint and palpation of the muscle
Oxford Scale 0 – No muscle contraction or movement seen or felt 1- Contraction felt or small movement seen 2- Joint able to move through full range , but only without the resistance of gravity 3- Joint able to move through full range with the resistance of gravity 4- Joint able to move through range against gravity and resistance 5- Normal Power
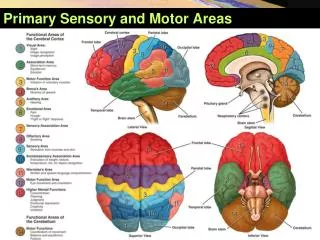
Co-ordination • Coordination is the ability to repeatedly execute a sequence of movements smoothly and accurately. • This may involve the senses, muscular contractions and joint movements. • Cerebellum in the brain is responsible for producing coordinated movements
Cerebellum • The cerebellum is involved in the coordination of voluntary motor movement, balance and equilibrium and muscle tone. It is located just above the brain stem and toward the back of the brain.
Testing Coordination • Hand to nose test • Heel to shin test • Aware of other factors influencing co-ordination:-muscle strength sensation proprioception
Sensory deficits Importance of sensation • Provides a feedback mechanism to allow appropriate postural and muscle adjustments to allow normal movement • Allows the recognition of objects without the need for vision • Prevents injury
Sensory Testing • Light touch • Pin prick • Hot / cold • Sensory Extinction • Proprioception • Two Point Discrimination • Stereognosis
Sensation The hand has several advantages over the eye; it can see in the dark and it can see round corners; most of all it can interact with the environment, rather than just observe it Porter and Lemon 1995
Practical In Groups Tasks one handed Recognising objects with reduced sensation Walking with an heavy leg Tasks with lack of sensation
References • Raine S, Meadows L, Lynch-Ellerington M (2009) Bobath concept theory and clinical practice in neurological rehabilitation 1st edition UK Wiley-Blackwell • Raine S. (2007) The current theoretical assumptions of the Bobath concept as determined by the members of BBTA. Physiotherapy Theory and Practice, 23:137-152. • Schumway- Cook A, Wollocott MH. (2007) Motor control translating research into clinical practice Third edition Philadelphia: Lippincott Williams & Wilkins.