Download
1 / 1
10 likes | 154 Views
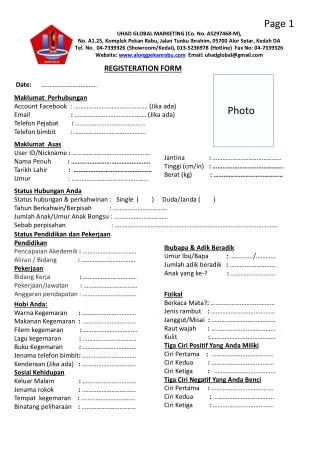
สำนักงานมูลนิธิ : อาคารคณะแพทยศาสตร์ มหาวิทยาลัยขอนแก่น เลขที่ 123 ถ.มิตรภาพ ต.ในเมือง อ.เมืองขอนแก่น จ.ขอนแก่น 40002 โทร. 081 1851151, 043 363123 โทรสาร 043 202558 http://www.tawanchai-foundation.org. มอบโอกาส วาดฝัน สร้างสรรค์รอยยิ้ม. แบบฟอร์มบริจาค / Donate form.

E N D
สำนักงานมูลนิธิ: อาคารคณะแพทยศาสตร์ มหาวิทยาลัยขอนแก่น เลขที่ 123 ถ.มิตรภาพ ต.ในเมือง อ.เมืองขอนแก่น จ.ขอนแก่น 40002 โทร. 081 1851151, 043 363123 โทรสาร 043 202558 http://www.tawanchai-foundation.org มอบโอกาส วาดฝัน สร้างสรรค์รอยยิ้ม แบบฟอร์มบริจาค / Donate form วันที่/Date............................................................................ ชื่อ-สกุล/Name…………………….....………………..............…………………………………………..………………………………..………….. ที่อยู่/Address……………………………………………………………………….……………………………………………………..……………… จังหวัด/Province………………………..…รหัสไปรษณีย์/Zip postal code……………………..ประเทศ/Country…………………….…โทรศัพท์/Phone……………………….…..…E-mail address..………………….....…………วันเกิด/Date of birth…………………….…………… ประสงค์บริจาค/Donation (….…..) เงินสด/Cash (……...) เช็ค/Chequeสาขา/Branch……………..…….……เลขที่/No…………………………..……วันที่/Date………………………… (……...) โอน/Transfer เข้าบัญชีมูลนิธิตะวันฉายเพื่อผู้ป่วยปากแหว่ง เพดานโหว่และพิการทางศีรษะและใบหน้า ธนาคารไทยพาณิชย์ สาขามหาวิทยาลัยขอนแก่น บัญชีเลขที่ 551 412873 0 (to SCB Bank, account number 551 412873 0) จำนวน/Amount Bath……………..บาท (.....................................................) ลงชื่อ/Sign………………………………ผู้บริจาค/Donator (..........................................................) หากประสงค์รับใบเสร็จรับเงินกรุณานำเงินสดหรือเช็คใส่ซองปิดผนึก กรณีโอนเงินกรุณาส่ง fax ใบนำฝากมาที่ 043 202558 (If you would like a receipt, please put cash or cheque into envelope. On transfer, please confirm your paymentby fax at 6643 202558) หากประสงค์บริจาคสิ่งของเพื่อเด็กและครอบครัวโปรดติดต่อมูลนิธิโดยตรง (If you would like to donate any other for children&family, please contact to office) ขอขอบพระคุณ / Thank You