Download
1 / 26
260 likes | 272 Views
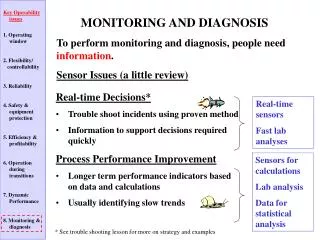
HIV Genetic Diversity Consequences for diagnosis, viral load and treatment monitoring Prof François SIMON François SIMON & Jean - Christophe PLANTIER University Par i s D i derot - Hospital Saint Louis – Paris 10. HIV GENETIC DIVERSITY : FROM SIV TO HIV.

E N D
HIV Genetic Diversity Consequences for diagnosis, viral load and treatment monitoring Prof François SIMON François SIMON & Jean - Christophe PLANTIER University Paris Diderot - Hospital Saint Louis – Paris 10
HIV GENETIC DIVERSITY : FROM SIV TO HIV • Different cross–species transmission events in the recent past - Two types : HIV1 & HIV2 - 4 HIV-1 groups (M, N, O & P) and 9 HIV2 groups (A to I) • Different HIV-1 group M subtypes (A to K) • High rate of HIV super/dual infections and HIV recombinant strains Increasing number of HIV-1 group M Circulating Recombinant Forms (CRF) and M- O inter group recombinant and HIV-2 inter-group recombinant strains • High replication - Volatile genome in host, high rate of mutations - Low genetic barrier against anti-retroviral and immune-responses
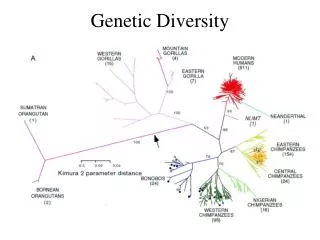
THE ORIGINS OF SIV/HIV : RECOMBINATION & INTER-SPECIES TRANSMISSIONS HIV-2 groups A to I HIV-1 groups M,N mnd2 mnd1 HIV-1 groups O, P Adapted from P Sharp, B Hahn, Cold Spring Harb Perspect Med 2011;1: a006841
REPLICATIVE FITNESS AND HIV-1 GENETIC DIVERSITY • High replication = high rate of mutations • Lowgeneticbarrieragainstanti-retroviral and immune- responses Ariën et al. Nature Reviews Microbiology 5 (February 2007) |
G r o u p M Group N Group P Group O HIV-1 GENETIC DIVERSITY IN 2016 Subtypes A-K 80 CRF Non M : NOP
HIV-1 NON- GROUP M GENETIC DIVERSITY IN 2016 Mourez et al CMR 2013
ESTIMATION OF MRCA S : THE EXEMPLE OF HIV-O DIFFERENT VIROLOGICAL AND EPIDEMIOLOGICAL WAVES 1970 1950 1930 Marginal posterior density courves obtained using 4 different population growth models Marie Leos, Plos Pathogen, 2015.
HIV-O MAIN CHARACTERISTICS • 1% of HIV-infected patients in Cameroon 143 cases diagnosed in France mainly in Cameroonian Pts • Pathogenic, sexual and vertical transmission documented • Lower replicativity than HIV-1 group M • 70% of the HIV-O are naturally resistant (Y181C) to NNRTI according to the phylogenetic position • Sensitive to enfuvirtide in vitro and in vivo despite N42D in 100%
HIV-N MAIN CHARACTERISTICS • Group N is close from the SIV cpz : cross species transmission occurring in the last decades • Pathogenic, sexual and vertical transmission documented • Low prevalence but strain trafficking outside of Cameroon, in Europe • Sensitive to all the ARV like group M strains • Low epidemic (to date) • a lower transmission rate ?
A B HIV-2 INFECTION : A COMPLEX MONITORING • HIV-2 is less pathogenic than HIV-1 with a slower decline in CD4 count • Lower replication : 50 % have “undetectable” plasma RNA (<100 copies/ml) • Not specific commercial HIV-2 Viral Load assays • Naturally resistant to NNRTI (including etravirine et rilpivirine) and fusion inhibitor enfuvirtide • Less sensitive to amprenavir, atazanavir in vitro • Sensitive to maraviroc, raltegravir, elvitegravir, dolutegravir • Poorest CD4 response = HAART must be initiated as early as 500 CD4 cells/mL
HIV-1 GROUP MAJOR M : GENETIC DIVERSITY IN 2016 http://clinicalgate.com/human-immunodeficiency-virus
HIV-1 GROUP M DIVERSITY IN AFRICA CRF02_AG Mali IvoryCoast Cameroon Congo Gabon Senegal English speaking countries : Subtype C D G FC Javaugue
HIV-1 group M diversityMain consequencesin 2016 Detection of HIV-1 non B duringprimary infection Viral Load miss-identification Drug sensitivity
VIROLOGICAL LIMITATIONS IN HIV SCREENING IN 2016 HIV-1 ANTIGENIC DIVERSITY • Highly divergent strains are circulating in Central • Africa and elsewhere • Ab not always fairly detected by all the screening assays • Different non-B p24 antigen epitopes • Up to 6 months following the seroconversion, antibodies have a low binding avidity to the antigen • RDTs lack of sensitivity during AHI • Follow-up of childrenborn to HIV seropositivemothersmainlyafter HAART initiation : false negativityin RTD
McCord Hospital outpatient department Acute HIV screening study, Durban, South Africa 994 RAPID TESTS NEGATIVE OR DISCORDANT, OUT PATIENTS AHI = 1% percent of outpatients with negative or discordant detectable through pooled serum HIV RNA screening. Bassett IV,HIV Med. 2011 AHI in adult population presenting fever ; Southern Mozambique 37.8% ( 32.7–43.2) of adults had undiagnosed established HIV infection. Serna-Bolea Celia , AIDS 2010 AHI = 3.3% ( 1.3–6.7 ) Acute HIV-1 infection is as common as malaria in coastal Kenya 3602 adults , HIV-1 prevalence 3.9% AHI in 5 of 506 HIV-1-negative or discordant patients Eduard J. Sanders, AIDS2014
LACK OF SCREENING TEST SENSITIVITY DURING HIV-1 NON-SUBTYPE B SEROCONVERSIONS 0.84±0.31 0.94±0.35 0.84±0.31 0.94±0.35 0.84±0.31 0.94±0.35 0.84±0.31 0.94±0.35 B Non-B Non-B B B Non-B Optical densitiy 4.52±4.3 0.91±1.21 4.52±4.3 EIA SANDWICH EIA INDIRECT 12subtype B vs 9 ‘non-B’ During early primary infection New EIA Sandwich : Increasing sensitivty for anti-subtype B antibodies only C Apetrei , AIDS 1996
HIV RAPID DIAGNOSTIC TESTS LACK OF SENSITIVITY DURING PRIMARY INFECTION Saint Louis Hospital , Paris : evaluation of 5 RDT EC-approved on the whole blood Prospective study, 200 HIV–1 B & non-B infected-patients • 3 acute primary infections (subtype B-2 and F-1) : 5/5 RTD negative • 1 HIV-1 group O-infected patient : 3/5 RDT negative Pavie, PlosOne 2010
p24 ANTIGENIC DIVERSITY DIVERSITY AND THE 1st COMBO FOURTH-GENERATION Ag-Ab RAPID TEST Combo Rapid Test : Lack of Antigen p24 Detection Supernatants of VariousSubtypes S Laperche , JID 2012
VIRAL LOAD ASSAYS AND HIV DIVERSITY IN 2016 • 20 years for viral load • Previously based only onto subtype B quantification • High sensitivity performances (LOD 20 copies/mL) • Overpassing (now) the genomic diversity • Random, Automation high throughput or unitary
IN 2001bDNA QUANTIPLEX 3.0 IN HIV-1 NON-B INFECTED PATIENTS WITH UNEXPECTEDLY LOW VIRAL LOAD ON MONITOR ROCHE Elizabeth R. Jenny-Avital, and Sara T. Beatrice Clin Infect Dis. 2001;32:1227-1230
IN 2016 RNA VIRAL LOAD ASSAYS ARE OVERPASSING THE HIV-1 GENOME DIVERSITY Subtypes HIV-1 viral Load : quality control , ANRS ANRS 2013
COMPARISON OF 4 VIRAL LOAD ASSAYS , PLASMA PANEL samples samples PANEL JC Plantier 2014
VIRAL LOAD AND HIV DIVERSITY : FROM 1996 TO 2016 • To survey the emergence of resistance • Rare but real discrepancies between the different assays whatever the subtype • Improved sensitivity for the large HIV-1group M diversity (B and non B) • Often, adapted to DBS and to DNA detection Discrepancies between a low viral load /failure of genotyping and low CD4 number suggestive of HIV variant
HIV- 1 GROUP M NON-B SUBTYPES ACQUIRED RESISTANCE TO ARV Active sites for polymerase and integrase are highly –conserved Subtype C propensity for K65R TDF-associated resistance mutation : limited consequences ( E White JID 2016) Etravirine & Rilpivirine : 10 % non-B strains harbour a mutation present in the HIV-1 subtype B score for resistance Natural polymorphism overlapping the acquired mutation againts PI Anti-integrase resistance profiles similar whatever the subtypes
HIV DIVERGENT STRAINS • CONSEQUENCES IN DIAGNOSIS & MONITORING • (HIV-1 group M non B, non M) • - Potential lack of sensitivity of the • screening assays during AHI with RDT • WB atypical profile (non B, non M) • Children born to HIV mothers Groups N-O- P, inter-Group M/O and HIV-2 - Different cross-species transmissions - trafficking in human population with a low prevalence - differences in pathogenicity HIV-2 and HIV-O natural resistance to non-nucleoside inhibitors HAART against HIV-2 must be initiated as early as 500 CD4 cells/mL • HIV-1 group B & non B, non M • Limitation in monitoring by molecular assays • - Need of viral load assay adapted • - Genotyping : failure of sequencing
HIV diversity is underlining the need for a rigorousepidemiological monitoring around the world François SIMON CHU saint Louis- Paris- France Jean-Christophe PLANTIER Marie LEOZ CHU Charles Nicolle, Rouen France Cristian APETREI University of Pittsburgh - USA