Download
1 / 21
210 likes | 366 Views
IPCP Core C Activities Aprepitant Dose-exposure Relationship in the Monkey. Jeffrey S. Barrett, Ph.D., FCP The Children’s Hospital of Philadelphia Division of Clinical Pharmacology and Therapeutics The University of Pennsylvania Medical School Department of Pediatrics.

E N D
IPCP Core C ActivitiesAprepitant Dose-exposure Relationship in the Monkey Jeffrey S. Barrett, Ph.D., FCPThe Children’s Hospital of PhiladelphiaDivision of Clinical Pharmacology and TherapeuticsThe University of Pennsylvania Medical SchoolDepartment of Pediatrics
IPCP Core C ActivitiesOutline • Background • Relevance of PK, PK/PD and M&S to IPCP • Overall grant strategy – M&S • M&S Integration with Decision Making • Aprepitant Review • PK Signature • Dose-selection rationale for CINV • PK Assessment – Suggestions for CDP • Current Core C Efforts • Analytical Methods • CFAR Pilot PK Results • Collaborative Efforts • SIV Dose Prediction • SIV Dose Prediction SIV PK/PD Projection to HIV • Analytical Effort • “Druggability” / Screening Criteria
IPCP Core C ActivitiesBackground – What we promised . . . • An evaluation of the correlation between single agent activity experiments and druggability properties theorized to benefit HAART. • An evaluation of the ability to generalize activity based on structural similarities of investigated agents. • Correlation of non-human primate to human pharmacokinetics via allometric modeling in order to guide clinical dosing based on pharmacokinetic considerations. Correlation of drug exposure to specific agent toxicities in non-human primates. • Construction of human PK/PD models built from in vitro, animal PK/PD and assumptions about human activity (efficacy and toxicity). • Correlation of non-human primate to patient exposure-response relationships. • Clinical trial simulation models to evaluate trial design sensitivities, drug combination and dosing scenarios and population characteristic dependencies.
IPCP Core C ActivitiesBackground – What we promised . . . PK (NCA) of aprepitant in HIV-infected patients (2-stage approach) Cross-validate aprepitant LC/MS/MS method (Constanzer et. al., 2004) • Population PK Model • (NLMEM) • Structural Model • Covariate Model • Error Model • Validation (data splitting or bootstrapping) Individual predicted pop-PK from final model (MAP Bayesian) PD: Exposure-response Safety Indices (Logistic Regression) PD: Exposure-response Psychologic Disturbances (Categorical Analysis) PD: Exposure-Response Viral Dynamics (NLMEM) PD: Exposure-Response NK response (NLMEM) Clinical Trial Simulation Model for Proof-of-Concept Phase IIA Trial
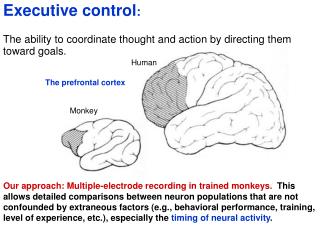
IPCP Core C ActivitiesRelevance of PK, PK/PD and M&S to IPCP
Aprepitant PK Characteristics Absorption • Mean absolute oral bioavailability of aprepitant is approximately 60 to 65% • Mean peak plasma concentration (Cmax) at approximately 4 hours (Tmax). • The pharmacokinetics of aprepitant are non-linear across the clinical dose range. • Increase in AUC0-∞ was 26% greater than dose proportional between 80-mg and 125-mg single doses administered in the fed state. Distribution • Aprepitant is greater than 95% bound to plasma proteins. The mean apparent volume of distribution at steady state (Vdss) is approximately 70 L in humans. Metabolism • Aprepitant undergoes extensive metabolism. • Metabolized primarily by CYP3A4 with minor metabolism by CYP1A2 and CYP2C19. Metabolism is largely via oxidation at the morpholine ring and its side chains. • No metabolism by CYP2D6, CYP2C9, or CYP2E1 detected. • Seven metabolites of aprepitant (weakly active) identified in human plasma. Excretion • Aprepitant is eliminated primarily by metabolism; not renally excreted. • The apparent plasma clearance of aprepitant ranged from approximately 62 to 90 mL/min. The apparent terminal half-life ranged from approximately 9 to 13 hours
125 mg 80 mg 80 mg Aprepitant PK Characteristics Time Postdose (hr) N=12
Aprepitant Dose SelectionCINV Indication • Correlation of aprepitant plasma trough concentration with binding of aprepitant to striatal NK1 receptors (each point represents an individual subject)
Analytical Methods • SFBC analysis / method – Monkey Plasma • Constanzer method (Merck); no IS • LOQ = 10 ng/mL • * CHOP / LAPKPD method for Monkey CSF
LC-MS/MS CSF Method *API 4000 mass spectrometry coupled w/ Alliance Waters HPLC * Electrospray ionization source * Positive ion mode * C18 Hypersil Column * Mobile phase (MP) a gradient MP of methanol and H2O with 0.1% formic acid * Multiple reaction monitoring at m/z 535.3 and 277.3 for aprepitant * Lowest of detection limit - 20 pg/mL
Time DG23 DF42 CB18 4/26/05 1.04 0.17 0.221 5/3/05 0.666 0.368 0.931 Pilot Study Results:Aprepitant in Rhesus Macaque Monkeys (n=3) CSF Levels (ng/mL)
Future Efforts: *Integrated model for aprepitant plasma – CSF exposure * Simulation PK/PD model to study regimens in SIV (cellular PD used as input to define target) *PK/PD in SIV * Scaling of SIV / HIV based on PK/PD * Implement FDA HIV disease model * Validate human analytical method at CHOP / LAPKPD
Recent FDA DiscussionTake Home Message *Tipranavir has more “warts” than aprepitant * Viral load reduction modest at best *FDA assisted with trial design, analysis and interpretation * Indication is focused on special population – treatment-resistant * Exposure-response indicates narrow therapeutic window * Many DDIs * Viability established on after numerous clinical evaluations