Download

1 / 61
610 likes | 633 Views
Insulin Resistance in Liver Diseases. Lt Col Prof Dr Shakeel Ahmed Mirza MBBS, MRCP ( UK ), FRCP ( London ) Classified Medical Specialist Gastroenterologist MH Rwp Hepatologist & Endocrinologist Prof of Medicine AFPGMI. Layout. What is Insulin Resistance ?

E N D
Insulin Resistance in Liver Diseases Lt Col Prof Dr Shakeel Ahmed Mirza MBBS, MRCP ( UK ), FRCP ( London ) Classified Medical Specialist Gastroenterologist MH Rwp Hepatologist & Endocrinologist Prof of Medicine AFPGMI
Layout • What is Insulin Resistance ? • What is mechanism of Insulin Resistance ? • Causes & its Relationship to • Obesity • Atherosclerosis • Hypertriglyceridemia • Epidemiology • Diagnosis • Management
Introduction The condition in which normal amounts of insulin are inadequate to produce a normal insulin response from fat, muscle and liver cells.
Insulin Resistance • Hyperinsulinemic individuals are at risk for developing Diabetes, Dyslipidemia, Hypertension & ultimately Cardiovascular disease • Patients with Metabolic Syndrome are 3.5 times as likely to die from Cardiovascular disease compared to normal people
Insulin Resistance • Hyperinsulinemia increases serum free fatty acid levels. • Chronic hyperinsulinemia promotes de novo hepatic lipogenesis • Activate profibrotic cytokines
Mechanism • It includes • Genetic or Primary target cell defects • Autoantibodies to insulin & • Accelerated insulin degradation
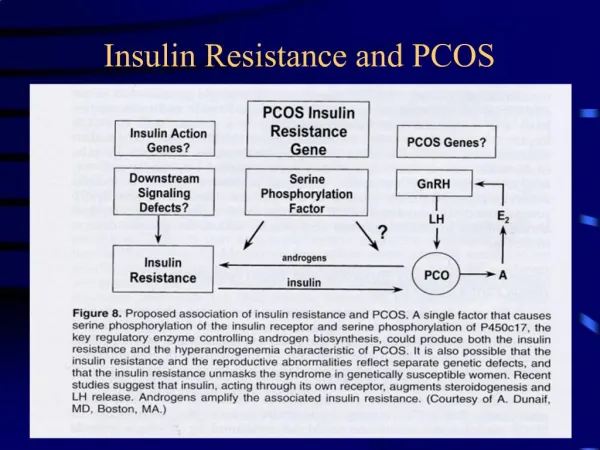
CAUSES of IR • Obesity • PCOD • Lipodystrophic states -. • Werner syndrome • Rabson-Mendenhall syndrome • Pineal hypertrophic syndrome • Immune insulin resistance • Low titer immunoglobulin (Ig) G anti-insulin antibodies are present in most patients receiving insulin. • Cushing syndrome and • Acromegaly
What Happens When Insulin Reaches Cells ? Insulin binding to IR will cause autophosphorylation and phosphorylation of IRS at Tyrosine, then IRS will be activated and bind to following components to activate the signal cascade. Glucose will be transport from blood into cells. Phosphorylation at Serine will block the IRS function.
GLUT4 Is The Transporter Of Glucose In Muscle And Adipose Tissue GLUT4 will be relocated from the cytoplasm to membrane Blue: DNA Red: GLUT4 Green: Transferon Foster et al, J. Biol. Chem., 2001
What Will Happen If GLUT4 Doesn’t move right? Insulin Resistance: An impaired biological response to insulin -Resistance to insulin-stimulated glucose uptake -Increased lipolysis/FFAs McFarlane SI, et al. J Clin Endocrinol Metab. 2001
Mechanisms Relating Insulin Resistance and Dyslipidemia Fat Cells Liver FFA X IR Insulin
Mechanisms Relating Insulin Resistance and Dyslipidemia Fat Cells Liver FFA TG Apo B VLDL VLDL X IR Insulin
Mechanisms Relating Insulin Resistance and Dyslipidemia Fat Cells Liver FFA CE (hepaticlipase) TG Apo B VLDL (CETP) HDL VLDL X IR TG Apo A-1 Kidney Insulin
Mechanisms Relating Insulin Resistance and Dyslipidemia Fat Cells Liver FFA CE (hepaticlipase) TG Apo B VLDL (CETP) HDL VLDL X IR TG Apo A-1 (CETP) CE TG Kidney Insulin SDLDL LDL (lipoprotein or hepatic lipase)
Relation Between Insulin Resistance and Hypertriglyceridemia 625 500 400 300 200 100 r = 0.73 P < 0.0001 Plasma TG (mg/dL) 100 200 300 400 500 600 Insulin Response to Oral Glucose* * Total area under 3-hour response curve (mean of 2 tests). Olefsky JM et al. AmJMed. 1974;57:551-560.
NAFLD • Fatty liver disease can range from fatty liver • alone (steatosis) • fatty liver associated with inflammation (steatohepatitis). • This condition can occur with the use of alcohol (alcohol-related fatty liver) or in the absence of alcohol (nonalcoholic fatty liver disease [NAFLD]).
What is NASH ?? Nonalcoholic steatohepatitis (NASH) is the term used to describe the distinct clinical entity in which patients lack a history of significant alcohol consumption but have liver biopsy findings indistinguishable from alcoholic steatohepatitis
NAFLD Epidemiology • Most common cause for elevated liver function tests in the United States due to the ongoing obesity epidemic in the United States. • Associated with the use of alcohol. This may occur with as little as 10 oz of alcohol ingested per week. Identical lesions also can be caused by other diseases or toxins.
Epidemiology • According to National Cholesterol Education Program Adult Treatment Panel III, insulin resistance syndrome is affecting about 24% of US adults aged greater than 20 years. • The syndrome is more common in older people and in Mexican Americans, and will increase in prevalence as populations age and become more obese
Epidemiology • It consists of the co-occurrence of metabolic risk factors for type 2 diabetes and cardiovascular disease , including • Overall obesity • Central obesity • Dyslipidemia • Hyperglycemia & • Hypertension.
Obesity • 60% of adults have BMI>25 (85th%) • 22% of adults have BMI>30 (95th%) • In 1990, there was no state with over 15% adults with BMI>30 • 25% of children have BMI over 85th% Lee, Arch Peds Ad Med, 162(7):682 July 2008
3.0 2.44 p for trend = 0.007 2.31 2.5 2.06 2.0 Relative risk 1.5 1.27 1.0 0.5 0.0 <69.8 69.8<74.2 74.2<79.2 79.2<86.3 86.3<139.7 Quintiles of waist circumference (cm) Abdominal obesity is linked to an increased risk of coronary heart disease Waist circumference has been shown to be independently associated with increased age-adjusted risk of CHD, even after adjusting for BMI and other cardiovascular risk factors CHD: coronary heart disease; BMI: body mass index Rexrode KM et al, 1998
Abdominal obesity increases the risk of developing type 2 diabetes 24 20 16 12 Relative risk 8 4 0 <71 71–75.9 76–81 81.1–86 86.1–91 91.1–96.3 >96.3 Waist circumference (cm) Carey VJ et al, 1997
CLINICAL PRESENTATION • Variable clinical presentation • Typically asymptomatic, but may have hepatomegaly and abdominal discomfort • Liver enzymes may be normal in >75% of cases, making them insensitive in detecting NAFLD • When increased, usually only modestly and limited to aminotransferases • ALT upper limits of normal: <30 in Male… • <20 in Female …..
HISTORY • History of weight fluctuations and if obese, for how long Document features of the metabolic syndrome (truncal obesity, HTN, low HDL, high TG, glucose intolerance) • Current and past medications • Family history of liver disease, diabetes,obesity
CLINICAL FEATURES • Fatigue • Malaise • A Dull Ache in upper right abdomen, a possible sign of an enlarged liver • Advance stage (e.g. cirrhosis) • Lack of appetite • Weight loss • Nausea • Easy Brusing • Weakness • Fatigue • Bleeding • Itching on Hands and Feet • Encephalopathy • Liver Failure
BIOCHEMICAL MARKERS • Serum ALT levels • Serum Gamma-glutamyltransferase (GGT) • Non-esterified fatty acids(NEFAs) • Glucose • Insulin resistance • Adiponectinlevels • Others
Lipids • Hyperlipidemia may be present. • Increased triglycerides are common in children and in patients with metabolic syndrome. • Iron studies • Elevations in serum ferritin, iron, and/or decreased transferrin saturation may occur in patients with NASH. • Although iron overload occurs in a small proportion of patients with NASH, these patients have more severe disease. • Viral serological markers: Before a diagnosis of NASH can be made, viral markers should be tested and viral infection excluded.
Autoimmune markers, such as antinuclear antibody (ANA) and anti–smooth muscle antibody (ASMA), are often slightly elevated in NASH. • Positive antibodies are associated with more severe fibrosis levels. • In the appropriate clinical setting, serum protein electrophoresis (SPEP) and anti–liver-kidney antibody may lead to a diagnosis of autoimmune liver disease. • Fasting insulin and glucose levels will alert the clinician to potential glucose intolerance and may lead to more effective therapies
OTHER NONINVASIVE TESTS Other noninvasive commercial tests for fibrosis (eg, FIBROSpect, FibroSURE, FibroScan) have not yet been proven in the Western population for NASH; however, large studies are ongoing.
Radiographic Studies • US : • Liver more echogenic than the R kidney • Spleen same density as the L kidney • CT : • Hypodense • Liver density less than the spleen • MRI : • Hypodense on the T2 image
US : NAFLD / NASH • Liver more echogenic than the R kidney • Spleen same density as the L kidney
DIAGNOSIS • Diagnosis of NAFLD can often be made by imaging stuAdies, including U/S, CT or MRI – detects presence of fat
DIAGNOSIS (cont.) • MR spectroscopy accurately measures hepatic triglyceride content • Has advantage over U/S, CT and MRI as it is quantitative rather than qualitative
CT Scan: NASH/NAFL • Hypodense • Liver density less than the spleen
MRI: NAFL / NASH Hypodense on the T2 image
MicrovesicularSteatosis • Central placed nucleus surround by numerous droplets • Acute condition with the impairment of fatty acid -oxidation • Poor prognosis, frequently death results
HISTOLOGY • Histologic evidence of steatohepatitis may disappear with progression to cirrhosis • Thus, significant proportion of cryptogenic cirrhosis is likely related to unrecognized NASH
MicrovesicularSteatosis • Acute fatty liver pregnancy • Jamaican vomiting sickness • Drugs • Aspirin • Valproic acid • Tetracyline • MDMA (ecstasy) • Ketoprofen • Amiodarone • Stavudine • Heat stroke • Reye’s syndrome • Metabolic • Urea cycle disorders • Mitochodrialcytopathies • Wolman’s disease • Cholesterol ester storage disease • Navajo neuropathy
MacrovesicularSteatosis • Nucleus displaced by single fat vacuole • Associations: • Obesity • Diabetes • Alcohol • Medications • Cachexia, rapid wt loss • Hepatitis C (genotype 3)
HISTOLOGY • Histologic diagnosis of NAFL requires presence of ≥ 5% steatosis • Indistinguishable from alcoholic fatty liver
Steatohepatitis (NASH) • Insulin resistance syndrome • Lipid abnormalities • Hyperlipidemia • Hypolipproteinemia • Rapid wt loss • Short bowel syndrome • Gastric bypass • Jejunal-ileal bypass • Lipodystrophy • TPN (choline deficiency) • Wilson’s • Drug induced
HISTOLOGY • NASH involves presence of steatosis with evidence of inflammation and hepatocyte injury: • Ballooning • Mallory bodies