Download
1 / 1
10 likes | 169 Views
“AN ATYPICAL CASE OF CONGESTIVE HEART FAILURE” M. BORGIA*, F. CIARAMELLA*, A. MAFFETTONE*, G. REA °, A. ASCIONE § and L. USSANO* *Cardio-Metabolic Medicine, “V. MONALDI” Hospital, AO OSPEDALI DEI COLLI, Naples ° Department of Radiology “V. MONALDI” Hospital, AO OSPEDALI DEI COLLI , Naples

E N D
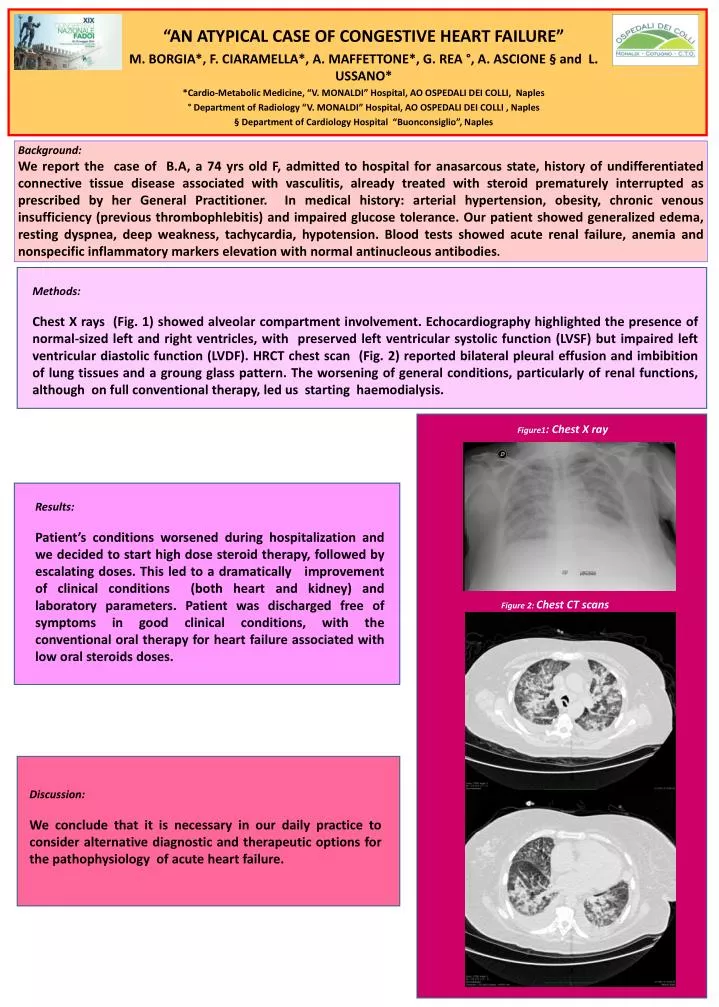
“AN ATYPICAL CASE OF CONGESTIVE HEART FAILURE” M. BORGIA*, F. CIARAMELLA*, A. MAFFETTONE*, G. REA °, A. ASCIONE § and L. USSANO* *Cardio-Metabolic Medicine, “V. MONALDI” Hospital, AO OSPEDALI DEI COLLI, Naples ° Department of Radiology “V. MONALDI”Hospital, AO OSPEDALI DEI COLLI , Naples § Department of Cardiology Hospital “Buonconsiglio”, Naples Background: We report the case of B.A, a 74 yrs old F, admitted to hospital for anasarcous state, history of undifferentiated connective tissue disease associated with vasculitis, already treated with steroid prematurely interrupted as prescribed by her General Practitioner. In medical history: arterial hypertension, obesity, chronic venous insufficiency (previous thrombophlebitis) and impaired glucose tolerance. Our patient showed generalized edema, resting dyspnea, deep weakness, tachycardia, hypotension. Blood tests showed acute renal failure, anemia and nonspecific inflammatory markers elevation with normal antinucleous antibodies. Methods: Chest X rays (Fig. 1) showed alveolar compartment involvement. Echocardiography highlighted the presence of normal-sized left and right ventricles, with preserved left ventricular systolic function (LVSF) but impaired left ventricular diastolic function (LVDF). HRCT chest scan (Fig. 2) reported bilateral pleural effusion and imbibition of lung tissues and a groung glass pattern. The worsening of general conditions, particularly of renal functions, although on full conventional therapy, led us starting haemodialysis. Figure1: Chest X ray Results: Patient’s conditions worsened during hospitalization and we decided to start high dose steroid therapy, followed by escalating doses. This led to a dramatically improvement of clinical conditions (both heart and kidney) and laboratory parameters. Patient was discharged free of symptoms in good clinical conditions, with the conventional oral therapy for heart failure associated with low oral steroids doses. Figure 2: Chest CT scans Discussion: We conclude that it is necessary in our daily practice to consider alternative diagnostic and therapeutic options for the pathophysiology of acute heart failure.