Download
1 / 19
370 likes | 1.61k Views
Parapneumonic Effusions and Empyema. Journal Club Preethi Yeturu and Navneesh Sharma February 18, 2009. Pleural Effusions. Abnormal accumulation of fluid in the pleural space due to a disruption of the equilibrium across pleural membranes Normal pleural fluid clear ultrafiltrate of plasma

E N D
Parapneumonic Effusions and Empyema Journal Club Preethi Yeturu and Navneesh Sharma February 18, 2009
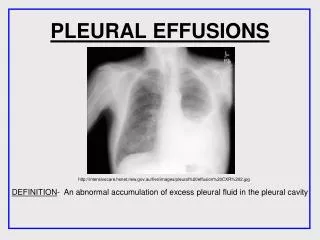
Pleural Effusions • Abnormal accumulation of fluid in the pleural space due to a disruption of the equilibrium across pleural membranes • Normal pleural fluid • clear ultrafiltrate of plasma • pH 7.6 - 7.64 • Protein content <2%, WBC <1000 • LDH <50% of plasma LDH • Two types • Transudate • Exudate
Transudate • Increased capillary hydrostatic pressure or decreased colloid oncotic pressure • Pleural membranes intact • Permiability of capillary membranes normal • Fluid is an ultrafiltrate of plasma • Causes • CHF • Cirrhosis • Nephritic syndrome
Exudate • Altered permeability of pleural membranes and capillaries or obstruction of lymphatic drainage of pleural space • Light’s criteria: one or more of following must be present • Pleural fluid/serum protein >0.5 • Pleural fluid/serum LDH>0.6 • Pleural fluid specific gravity >1.018 • Causes • Parapneumonic • TB • Malignancy • PE
Parapneumonic Effusions • Any pleural effusion associated with bacterial pneumonia, lung abscess or bronchiectasis • Most common cause of exudative pleural effusions in US • 40-60% of bacterial pneumonias result in pleural effusions • Three types • Uncomplicated parapneumonic effusion • Complicated parapneumonic effusion • Empyema
Uncomplicated Effusions • Parenchymal infection leads to increased interstitial fluid that causes accumulation of sterile pleural effusion • Pleural fluid is often small (<10mm) • sterile w/ small amount of PMNs • glucose and pH wnl • Resolve with resolution of pneumonia and treatment w/ antibiotics
Complicated Effusions • Persistent bacterial infection of previously sterile pleural fluid • Pleural fluid • Many PMNs, bacteria and cell debris • Acidosis - pH and glucose decrease • LDH increases • Possible deposition of fibrin on pleura - formation of multiple locules
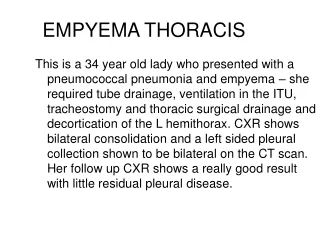
Empyema • Characterized by bacteria seen on gram stain or aspiration of pus • 60% from complicated parapneumonic effusions • 20% after thoracic surgery • Pleural fluid • Possible formation of pleural peel that can encase the lung and hinder reexpansion
Clinical Manifestations • History • Acute febrile episode • Dyspnea • Cough - w/ purulent sputum • Pleuritic chest pain • Weight loss • Physical exam • Dullness to percussion • Diminished breath sounds in affected hemithorax • Decreased tactile fremitus • Egophony • Pleuritic friction rub
Diagnosis - Imaging CXR • blunting of costrophrenic angle on upright films • Lateral decubitus films - better view of subpulmonic effusions, show if effusion is freely-flowing, thickness of effusion
Diagnosis - Imaging CT - w/ IV contrast is optimal • Allow for differentiation betwn parenchymal and pleural disease • Contrast enhances pleural surface
Diagnosis • Thoracentesis • Sample if any of following are present • Free flowing but >10mm in lateral decubitus film • Loculated • Associated w/ thickened parietal pleura on CT - suggests empyema • Complications - pain, bleeding, pneumothorax, puncture of liver or spleen
Analysis of Pleural Fluid • Gross examination for color, turbidity and odor • Microbiology - gram stain and cultures • pH or glucose, LDH, protein • CBC w/ differential
Analysis of Pleural Fluid • Characteristics of Pleural Fluid
Treatment • Depends on type and category of effusion • Uncomplicated - category 1 or 2 • Resolves w/ antibiotic treatment alone • Does not need drainage • Complicated - category 3 • Variable response to antibiotics alone - thus often treated like empyema • Empyema - category 4 • Requires complete drainage • Goal of therapy: • Sterilization of cavity - antibiotics for 4-6 weeks • Complete drainage as evidenced by minimal chest tube output and CT documentation that no residual loculations persist • Obliteration of empyema cavity w/ adequate lung expansion
Drainage of Effusion • Theurapeutic thoracentesis • Tube thoracotomy • Often left until rate of drainage <50mL/day and cavity is closed • W/ fibrinolytics - intrapleural administration was suggested for loculated effusions • Reported data does not demonstrate benefit in most pts • Thoracoscopy • Alternative treatment for multiloculated empyema • Open thoracostomy • Open drainage at inferior border of empyema cavity w/ chest tube • Preferred in pts who cannot tolerate thoracotomy
Drainage of Effusion • Thoracotomy w/ decortication • For pts who require additional drainage after trial of tube thoracostomy and thoracoscopy • Or pt who have fibrin deposition that hinders ability of lung to expand