Download
1 / 41
430 likes | 755 Views
Estrogens. Chemistry Natural estrogens 17- β -estradiol, estrone, estriol Equine estrogens: equilenin, equilin Synthetic estrogens Steroidal:Ethinyl estradiol, mestranol, quinestrol Non-steroidal: diethylstilbestrol (DES), chlortrianisen, methllenstril Phytoestrogens: flavonoids (soybeans)

E N D
Estrogens Chemistry Natural estrogens 17-β-estradiol, estrone, estriol Equine estrogens: equilenin, equilin Synthetic estrogens Steroidal:Ethinyl estradiol, mestranol, quinestrol Non-steroidal: diethylstilbestrol (DES), chlortrianisen, methllenstril Phytoestrogens: flavonoids (soybeans) Bisphenols, phatalate phenols in plastics
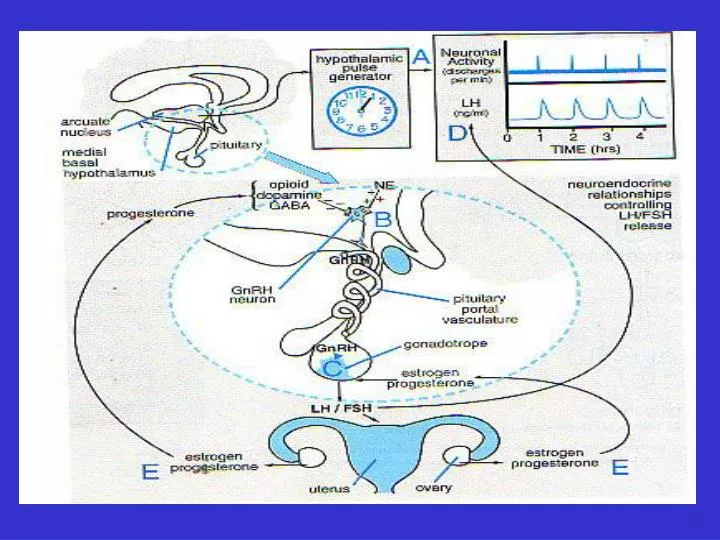
Biosynthesis • Premenopause women Major source are ovareis: E2, E1, E3 • Pregnant women A large amount of estrogens are produced by fetoplacental unit • Menopause women Estrone synthesize from dehydroepiandrosterone in adipose tissue
Pharmacokinetics • Various estrogens are available oral, parenteral, tramsdermal, topical • Natural estrogens have FPM • Natural estrogens bound mainly to SHBG and lesser to albumin in contrast to synthetic agents • Metabolize in liver and excrete in urine and feces (enterohepatic cycle) • 50-850 pg/ml
Mechanism of action • Two type, α and β, of receptors which are members of the superfamily of steroids Sterol, retinoic acid, and thyroid. • The receptor-hormone complex bound to EREs! • However, there is some rapid estrogen-induced effects.
Physiologic effects 1. Female maturation 2. Endometrial effects 3. Metabolic and cardiovascular effects on: Blood vessels, skin, bone resorption, leptin, CBG, TBG, SHBG, transferin, renin substrate, fibrinogen,HDL, LDL, TG 4. effects on blood coagulation 5. other effects Induction of progesterone receptors synthesis, stimulating the production of CRH, sympathetic system, well being in estrogen-deficient women, edema, sodium and water retention.
Clinical Uses 1. Primary hypogonadism 2. Postmenopausal Hormonal Therapy Loss of periods, vasomotor symptoms, sleep disturbances, genital atrophy, bone loss, lipid changes,CVD 3. Intractable dysmenorrhea (with progestins) 4. Hirsutism and amenorrhea due to high androgens
Postmenopausal Hormone Replacement Therapy • Careful assessment of case symptoms • Consideration of her age • Presence of (or risk) cardiovascular disease, osteoporosis, breast cancer, endometrial cancer • Goal of therapy • Risk of therapy • Discuss with patient
A large study from WHI project showing no CV benefit from estrogen plus progestin replacement therapy in perimenopausal or older postmenopausal patients.
Adverse effects 1. uterine bleeding 2. cancer 3. nausea 4. breast tenderness 5. hyperpigmentation 6. migraine 7. Cholestasis 8. gallbladder disease 9. hypertension
Contraindication • Estrogen dependent neoplasm • Undiagnosed genital bleeding • Liver disease • History of thromboembolic disorder • Heavy smokers!
Estrogens inhibitors • SERMs (selective estrogen receptor modulators) They have agonistic action in some tissues and antagonistic properties in others. Tamoxifen: • A competitive Partial agonist at estrogen receptors • was the first SERMs • Extensively use for palliative treatment of breast cancer in postmenopause and high risk women • Orally given • T1/2 7-14 hrs • 10-20 mg twice daily • Predominantly excretes trough liver • Hot flushes, nausea, vomiting, occur in 25% of cases • Has agonist activity at bone and uterus! :
Raloxifene: • Is an another SERMs • Agonistic effects on lipid and bone • Antagonistic effects on uterus and breast • Has FPM, long t1/2 (>24), high Vd • Approved for prevention of postmenopausal osteoporosis
Clomiphene: • Has a weak estrogen activity • Act as inhibitor of endogenous estrogen • Block endogenous estrogen’s negative feed back on gonadotrophins • Use in treatment of disorders of ovulation (PCOS) • Single ovulation with single course of therapy • In ovarian or pituitary failure?! • 100 mg/day for 5 days
Adverse effects: hot flushes, afterimage, headache, constipation, allergic reactions, reversible hair loss, enlarged ovary, nausea, vomiting, increased nervous tension, depression, fatigue, breast soreness, weight gain, urinary frequency, heavy menses, multiple pregnancy (10%) Cautions: In cases with enlarged ovary (small doses), cases with complain of abdominal symptoms (examined carefully), visual symptoms
Aromatase inhibitors Anastrozole, Letrozole (reversible) Exemestane (irreversible) Approved for advance breast cancer • Antagonists Fulvestrant Cases who have resistant to tamoxifen
Progestins Chemistry Natural Progesterone Synthetic Progesterone derivatives: Hydroxyprogesterone, medroxyprogesterone, megesterol 17-ethinyltestosterone derivatives: Dimethisterone 19-nortestosterone: Desogestrel, norethynodrel, lynestrenol, norethindrone, L-norgestrel • Biosynthesis
Pharmacokinetics Progesterone Rapidly absorbed, plasma half life 5min, almost completely metabolized in liver (pregnanediol), Progesterone bound to albumin, 19-nor bound to SHBG and albumin, MPA bound to albumin There is some IM preparation Synthetics have longer half life, e.g. 7 hrs for norethindrone • Mechanism of Action
Physiologic Effects Metabolic: • Little effect on protein, stimulate LPL, increase basal insulin levels and insulin response to glucose, promote glycogen storage, promote ketogenesis • Endocrine: Compete with aldosterone, participate in LH surge, maturation and secretory change in endometrium CNS: • Increase body temperature, increase response to CO2, depression, hypnosis Exocrine: • Alveolar development,
Clinical Uses 1.HRT 2. Contraception 3. endometriosis 4. dysmenorrhea 5. PMHRT 6. PMS! 7. Diagnostic use
Adverse effects • Hypertension • Decrease HDL (More androgenic agents) • Risk of breast cancer!
Progesterone inhibitors Mifepristone (RU486) • Is a 19-norsteroid • Is a competitive antagonist at progesterone and glucocorticoids receptors • Has luteolytic properties Pharmacokinetics: • Long half life Clinical use: • Postcoital contraception • Endometrosis • Cushing’s syndrome • Breast cancer • Meningiomas • Termination of early pregnancies Adverse effect
Contraception • In women 1. combination of estrogen and progesterone (monophasic, biphasic, triphasic) 2. Continuous progestin therapy without estrogens • Mechanism of action: Inhibition of ovulation Changes in cervical mucus Changes in motility and secretion of uterine tubes Changes in endometrium
Adverse Effects • Mild Nausea, mastalgia, breakthrough bleeding, edema, changes in serum protein, increase ESR, headache, withdrawal bleeding fails • Moderate Breakthrough bleeding, weight gain, pigmentation, acne, hirsutism, urethral dilation, vaginal infection • Severe Vascular disorder, MI, stroke, cholestatic jaundice, depression, cancer
Androgens and Anabolic Steroids • In male, the most important androgen secreted by the testis is testosterone Biosynthesis: Similar to those occur in adrenal and ovary secret 8 mg/D, 95% by leydig cells, 5% by adrenal Testis also secret another less potent androgens: dehydroepiandrosterone, androstenedione; and a more potent agent dihydrotestosterone Plasma levels in male at puberty 0.6 mcg/dl, in female 0.03 mcg/dl (from ovary and adrenal and peripheral conversion of other compounds)
Protein binding SHBG (65%), 2% is free and remaining bound to albumin • Metabolism In many tissues convert to dihydrotestosterone by 5α-reductase In some tissues convert to estrogen by P450 aromatase (liver, hypothalamus, adipose tissue) Major degradation pathway of testostrone occur in liver: androstrone, ethiochoanolone
Physiologic effects • Changes in puberty of normal male: General growth-promoting effects on body tissues and sexual organs Appearance of pubic, auxiliary, and beard hair. Activation of sebaceous glands Epiphysial closure and bone growth stimulate • Stimulation and maintaining sexual function • Reduction of binding and carrier proteins • Increase the clotting factors, triglyceride lipase, antitripsin, haptoglobulin, sialic acid • Stimulate erythropoietin, decrease HDL
Synthetic Androgens and Anabolics • As other sex steroids has low oral bioavailability Ester forms: Testosterone cypionate, undecanoate, enanthate, propionate Alkylated at 17 position: Methyltestosterone, fluxymesterone, oxymetholone,
Pharmacologic effects • In adult male: suppress gonadotrophins and atrophy of testis • Virilism • Feminism • Erythropoesis • Anabolic effects
Clinical uses • Replacement therapy • Breast engorgement during postpartum period (with estrogens) • Endometriosis (Danazol) • Breast tumors in premenopausal women • PHRT • For induction of anabolic effects in some situations • Anemia • Osteoporosis • In aging
Adverse effects • Masculinizing (women and children) • In women: hirsutism, acne, amenorrhea, clitoral enlargement, deepening of the voice, progestational effects!, increase susceptibility to atherosclerosis • Edema • Liver dysfunction! • Prostatic hypereplasia • Psychotic symptoms
contraindication • In pregnant women • In carcinoma of prostate and male breast cancer • Infant and young children
Antiandrogens • Steroid Synthesis Inhibition Ketoconazole • Is an antifungal • Also, is an inhibitor of adrenal and gonadal steroid inhibitor • Inhibits the cholesterol side chain cleavage • It does not affect ovarian but decrease placental aromatase activity • It displaces estradiol and dihydrotestosterone from SHBG in vitro • It increases the estradiol/testosterone ration in vivo • Clinical Use?!!
Inhibitors of testosterone conversion • In prostate, skin, seminal vesicle, and epidiymis DHT is essential androgen • 5α-reductase Finasteride • a steroid-like inhibitor of 5α-reductase • Onset of action 8hrs, duration 24hrs • T1/2 8hrs (longer in geriatrics) • 50% metabolize and the rest excrete from feces • Clinical use: BPH (5 mg/d), baldness (1 mg/d)
Receptor Inhibitors Cyproterone, cyptroterone acetate • Cyproterone acetate has a marked progestational effect, So, has more antiandrogenic effect • They use to treat hirsutism in women and for excessive sex drive in men Flutamide • Is a potent competitive antiandrogenic • Rapidly metabolized in humans • Use in the treatment of prostatic carcinoma • Management of excess androgen effect in women • Adeverse effects: gynecomastia, mild reversible hepatic toxicity • Bicalutamide, nilutamide
Spironolactone Compete with DHT for androgen receptors Also, reduce 17α-hydroxylase activity, lowering plasmalevel of testosterone and androstendione 50-200 mg/d in hirsutism in women as effective as finastride, flutamide, or cyproterone