Download
1 / 1
10 likes | 172 Views
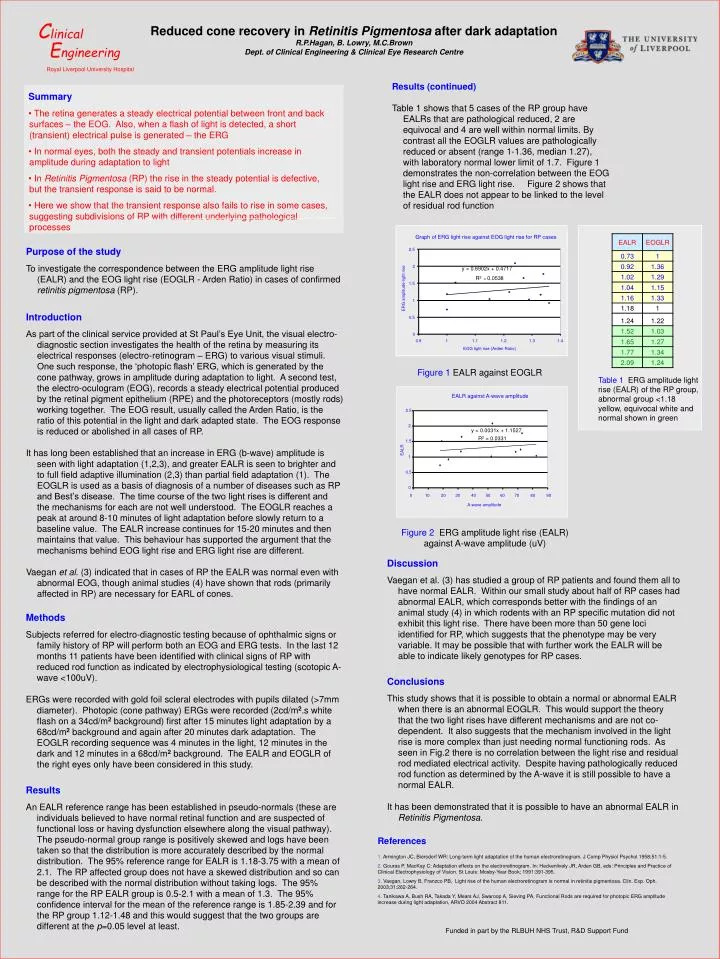
C linical. E ngineering. Royal Liverpool University Hospital. Reduced cone recovery in Retinitis Pigmentosa after dark adaptation R.P.Hagan, B. Lowry, M.C.Brown Dept. of Clinical Engineering & Clinical Eye Research Centre. Results (continued)

E N D
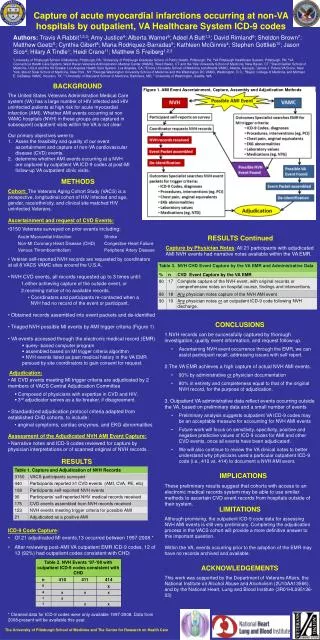
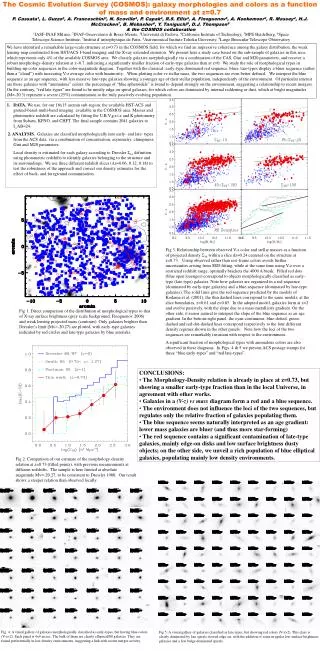
Clinical Engineering Royal Liverpool University Hospital Reduced cone recovery in Retinitis Pigmentosa after dark adaptation R.P.Hagan, B. Lowry, M.C.Brown Dept. of Clinical Engineering & Clinical Eye Research Centre Results (continued) Table 1 shows that 5 cases of the RP group have EALRs that are pathological reduced, 2 are equivocal and 4 are well within normal limits. By contrast all the EOGLR values are pathologically reduced or absent (range 1-1.36, median 1.27), with laboratory normal lower limit of 1.7. Figure 1 demonstrates the non-correlation between the EOG light rise and ERG light rise. Figure 2 shows that the EALR does not appear to be linked to the level of residual rod function • Summary • The retina generates a steady electrical potential between front and back surfaces – the EOG. Also, when a flash of light is detected, a short (transient) electrical pulse is generated – the ERG • In normal eyes, both the steady and transient potentials increase in amplitude during adaptation to light • In Retinitis Pigmentosa (RP) the rise in the steady potential is defective, but the transient response is said to be normal. • Here we show that the transient response also fails to rise in some cases, suggesting subdivisions of RP with different underlying pathological processes Graph of ERG light rise against EOG light rise for RP cases Purpose of the study To investigate the correspondence between the ERG amplitude light rise (EALR) and the EOG light rise (EOGLR - Arden Ratio) in cases of confirmed retinitis pigmentosa (RP). 2.5 2 y = 0.6902x + 0.4717 R2 = 0.0538 1.5 ERG amplitude light rise 1 Introduction As part of the clinical service provided at St Paul’s Eye Unit, the visual electro-diagnostic section investigates the health of the retina by measuring its electrical responses (electro-retinogram – ERG) to various visual stimuli. One such response, the ‘photopic flash’ ERG, which is generated by the cone pathway, grows in amplitude during adaptation to light. A second test, the electro-oculogram (EOG), records a steady electrical potential produced by the retinal pigment epithelium (RPE) and the photoreceptors (mostly rods) working together. The EOG result, usually called the Arden Ratio, is the ratio of this potential in the light and dark adapted state. The EOG response is reduced or abolished in all cases of RP. It has long been established that an increase in ERG (b-wave) amplitude is seen with light adaptation (1,2,3), and greater EALR is seen to brighter and to full field adaptive illumination (2,3) than partial field adaptation (1). The EOGLR is used as a basis of diagnosis of a number of diseases such as RP and Best’s disease. The time course of the two light rises is different and the mechanisms for each are not well understood. The EOGLR reaches a peak at around 8-10 minutes of light adaptation before slowly return to a baseline value. The EALR increase continues for 15-20 minutes and then maintains that value. This behaviour has supported the argument that the mechanisms behind EOG light rise and ERG light rise are different. Vaegan et al. (3) indicated that in cases of RP the EALR was normal even with abnormal EOG, though animal studies (4) have shown that rods (primarily affected in RP) are necessary for EARL of cones. 0.5 0 0.9 1 1.1 1.2 1.3 1.4 EOG light rise (Arden Ratio) Figure 1 EALR against EOGLR Table 1 ERG amplitude light rise (EALR) of the RP group, abnormal group <1.18 yellow, equivocal white and normal shown in green EALR against A-wave amplitude 2.5 2 y = 0.0031x + 1.1527 R2 = 0.0331 1.5 EALR 1 0.5 0 0 10 20 30 40 50 60 70 80 90 A-wave amplitude Figure 2 ERG amplitude light rise (EALR) against A-wave amplitude (uV) Discussion Vaegan et al. (3) has studied a group of RP patients and found them all to have normal EALR. Within our small study about half of RP cases had abnormal EALR, which corresponds better with the findings of an animal study (4) in which rodents with an RP specific mutation did not exhibit this light rise. There have been more than 50 gene loci identified for RP, which suggests that the phenotype may be very variable. It may be possible that with further work the EALR will be able to indicate likely genotypes for RP cases. Methods Subjects referred for electro-diagnostic testing because of ophthalmic signs or family history of RP will perform both an EOG and ERG tests. In the last 12 months 11 patients have been identified with clinical signs of RP with reduced rod function as indicated by electrophysiological testing (scotopic A-wave <100uV). ERGs were recorded with gold foil scleral electrodes with pupils dilated (>7mm diameter). Photopic (cone pathway) ERGs were recorded (2cd/m2.s white flash on a 34cd/m2 background) first after 15 minutes light adaptation by a 68cd/m2 background and again after 20 minutes dark adaptation. The EOGLR recording sequence was 4 minutes in the light, 12 minutes in the dark and 12 minutes in a 68cd/m2 background. The EALR and EOGLR of the right eyes only have been considered in this study. Conclusions This study shows that it is possible to obtain a normal or abnormal EALR when there is an abnormal EOGLR. This would support the theory that the two light rises have different mechanisms and are not co-dependent. It also suggests that the mechanism involved in the light rise is more complex than just needing normal functioning rods. As seen in Fig.2 there is no correlation between the light rise and residual rod mediated electrical activity. Despite having pathologically reduced rod function as determined by the A-wave it is still possible to have a normal EALR. It has been demonstrated that it is possible to have an abnormal EALR in Retinitis Pigmentosa. Results An EALR reference range has been established in pseudo-normals (these are individuals believed to have normal retinal function and are suspected of functional loss or having dysfunction elsewhere along the visual pathway). The pseudo-normal group range is positively skewed and logs have been taken so that the distribution is more accurately described by the normal distribution. The 95% reference range for EALR is 1.18-3.75 with a mean of 2.1. The RP affected group does not have a skewed distribution and so can be described with the normal distribution without taking logs. The 95% range for the RP EALR group is 0.5-2.1 with a mean of 1.3. The 95% confidence interval for the mean of the reference range is 1.85-2.39 and for the RP group 1.12-1.48 and this would suggest that the two groups are different at the p=0.05 level at least. References 1. Armington JC, Biersdorf WR: Long-term light adaptation of the human electroretinogram. J Comp Physiol Psychol 1958;51:1-5. 2. Gouras P, MacKay C: Adaptation effects on the electroretinogram. In: Heckenlively JR, Arden GB, eds: Principles and Practice of Clinical Electrophysiology of Vision. St Louis: Mosby-Year Book; 1991:391-395. 3. Vaegan, Lowry B, Franzco PB, Light rise of the human electroretinogram is normal in retinitis pigmentosa. Clin. Exp. Oph. 2003;31:262-264. 4. Tanikawa A, Bush RA, Takada Y, Mears AJ, Swaroop A, Sieving PA, Functional Rods are required for photopic ERG amplitude increase during light adaptation, ARVO 2004 Abstract 811. Funded in part by the RLBUH NHS Trust, R&D Support Fund