Download
1 / 67
720 likes | 1.27k Views
Pericarditis & Myocarditis. April 6 th , 2006 Shawn Dowling. Objectives. Review Dx Tx ECG’s changes. Anatomy and Physiology. Parietal layer Thick, collagenous, stiff Adventitial attachments to sternum, diaphragm, mediastinum Visceral layer Thin Closely adherent to epicardial surface.

E N D
Pericarditis &Myocarditis April 6th, 2006 Shawn Dowling
Objectives • Review • Dx • Tx • ECG’s changes
Anatomy and Physiology • Parietal layer • Thick, collagenous, stiff • Adventitial attachments to sternum, diaphragm, mediastinum • Visceral layer • Thin • Closely adherent to epicardial surface
Pericardial Anatomy/Physiology • Pericardial space • Normally 15-60 cc fluid • Functions • Reduces friction • Prevention of infection • Augmentation of atrial filling & maintains normal pressure-volume relationship of chambers • But…No physiological consequence to absent pericardium
Case #1 • You’re working in the ED and have a patient that is sent in from their family doc with a diagnosis of perdicarditis (based on the history). He’s a 26 yo M. • Describe the classic symptoms of Pericarditis.
Hx: Sudden onset severe CP, x 24H Pleuritic, worsened w/lying flat Rads to back area No SOB, not exertional, no PND ROS: fevers, recent URTI Sx, PMHx: Otherwise healthy Meds: Tylenol for the pain – not really working Pericarditis - History
Pericarditis is… • An inflammation of the pericardium • IR 2-6%, adults>children, Male>female, • # of disease processes/agents responsible • Classic Dx is pleuritic CP, pericardial rub & ECG • Can have ischemic quality and positional component • For research purposes usually 2 of 3 • Usually benign condition, but there are a few complications • But, you need to consider a few very important Dx before diagnosing pericarditis
DDx to consider… • Pneumonia or pneumonitis with pleurisy • PE • Costochondritis • GERD • MI • Aortic dissection • Pneumothorax
You’re about to examine the patient when the your staff asks you • What physical examine finding is most helpful in making the diagnosis of pericarditis? • Does your inability to illicit this p/e finding rule out the disease?
Physical Exam • Looks to be in pain, not toxic looking • VS–HR 110,RR-12(98%),T – 38.7°, 138/75 • Cardiac: S1+,S2+, (link), JVP 2 ASA, no peripheral edema, PMI N. • Lungs – clear, no c or w, no WOB, shallow respirations • Rest of exam N
What’s that sound? • Mono-,Bi-,Tri-phasic Rub • Atrial systolic rub that precedes S1, • Ventricular systolic rub between S1 and S2 and coincident with the peak carotid pulse, and • Early diastolic rub after S2 (usually the faintest). • Best heard at LLSB, pt sitting forward • Intermittent and migratory (unlike murmur) • Spec 100%, Sens Poor
Investigations • What are you going to order? • Labs? • Imaging? • CV investigations?
Labs • WBC usually elevated • ESR usually elevated - do not order • Troponin • What does it signify if +ve? • Does this change disposition?
Imaging • CXR • CT scan • MRI Not our domain
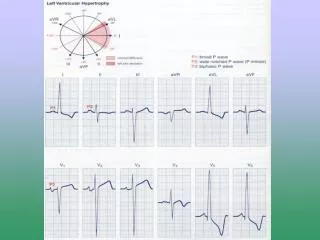
What phase of ECG changes are these? aVR PR segment PR (most specific) ST (diffuse, concave) What are the other phases?
ECG Findings of Pericarditis • What are the 4 phases of pericarditis? • Which findings are most specific? • The staging is not very helpful – but popular question to be asked
Stage 1 (hours days) • Hours to days (often only ECG findings since we Tx and pt may not progress to next stage) • Diffuse ST elevation • ventricular subepicardial injury • I, II, III, aVL, aVF, V2 to V6 • Concave upwards • No distinct J-point • No T-wave inversions • PR Elevation • aVR • Diffuse PR depression • atrial injury
Stage 2 (variable timeline) • ST / PR return to baseline • Some T-wave flattening Stage 3 (Variable timeline) • T-wave inversion • Deep, uniform
Stage 4 (Weeks to months) • Return to normal • Some patients may have residual T-wave inversion
But how do we distinguish these ST changes from BER? ST=PR-Jp pt T=J pt to peak of Twave
Pericarditis Concave STE <5mm No reciprocal STD ECG changes usually over hours to days AMI Convex Variable amt STE Often see reciprocal ECG can evolve very rapidly Pericarditis versus AMI
What is the significance of this ECG in the setting of his CXR? Criteria for this?
ECG Findings of Pericardial Effusion • When should a pericardiocentesis be done • Diagnostically – i.e. concerned about CA, TB, • Purulent Pericarditis • Unresponsive to treatment • Severe symptoms: SOBtamponade • Pericardectomy/window: Consider for traumatic hemopericardium and purulent pericarditis
Idiopathic Infectious Viral: enterovirus (MC), CMV, hepatitis B, infectious mononucleosis, HIV/AIDs) Bacterial (Pneumococcus, Staphylococcus, Streptococcus, Mycoplasma, Lyme disease, Hemophilus influenzae, Neisseria meningitidis) Mycobacteria (Mycobacterium tuberculosis, Mycobacterium avium-intracellulare) Immune-inflammatory Connective tissue disease(SLE, RA, scleroderma) Early post-myocardial infarction Late post-myocardial infarction (Dressler syndrome),late post-cardiotomy/thoracotomy, late post-trauma Drug induced(e.g., procainamide, hydralazine, isoniazid, cyclosporine) Neoplastic disease Secondary: breast and lung carcinoma, lymphomas, leukemias Radiation induced Trauma Blunt and penetrating,post-cardiopulmonary resuscitation Miscellaneous Chronic renal failure, dialysis related Hypothyroidism Amyloidosis Aortic dissection Etiology of pericarditis?
INFECTIOUS Viral Coxsackie, adeno, Echoviruses, HIV, mumps, EBV, etc. Bacterial Pneumococcus, Staphylococcus, Streptococcus, Mycoplasma, Lyme disease, Hemophilus influenzae, Neisseria meningitidis Fungal NON-INFECTIOUS IDIOPATHIC (MC) Traumatic Days to mths after Post-MI Early Late: Dressler’s Auto-immune dz: RA, SLE, vasculitides, sarcoid Malignant Post-irradiation Drug-induced Pericarditis - etiology
Pericarditis Acute Chronic (>3/12) Consider broad Ddx Usually inflammatory Recurrent Reasons to investigate further: 1)prolonged latent period before recurrence 2)presence of anti-heart antibodies (one way to have ER nurses hate ya – order anti-sarcollemmal/antifibirllary antibodies and keep pt in ED until results come back) 3)Rapid response to steroids in setting of auto-immune disease
Mainstay’s of Tx • Drugs • NSAID’s (level B, Class 1) • Mainstay of treatment for idiopathic/viral cause • Advil 600-800mg TID or ASA 650 QID • Indocid – avoid since some evidence of coronary flow • Duration: recommend x 2wks and discontinue once asymptomatic • Steroids – traditionally recommended, but some evidence that ↑ with stopping steroids
Viral/Idiopathic • MC cause of pericarditis • Tx: symptomatic treatment with ibuprofen 600mg PO TID until ASx or 2 wks, whichever comes first • ECHO? • if considerably symptomatic • ?pericardial effusion • If being admitted • Trop? • If concerned about ischemia • If concerned about Myocarditis • At your discretion (cardiologist here recommend trop in all cases of pericarditis to ensure no myocarditis)
Recurrent Pericarditis or Refractory to initial Tx • What other options do you have? • 1st line for recurrent • Colchicine (Adler) 2mg PO 1st day, then 0.5 BID until ASx • Prednisone (especially when underlying auto-immune process)
What do the (french) cardiologist do… • Survey of French cardiologist in 2005 • initial investigations ECG in 100% of cases, ECHO in 95%, b.w. in 93% of cases. • Hospitalisation was advised by only 24% of cardiologists. • Aspirin was prescribed as first choice treatment in 92.5% of cases. • Duration of treatment recommendations varied widely, from <5 days by 2.5%, between 5 and 10 days by 25.5%, 11 and 15 days by 23.0%, 16 to 21 days by 35.3%, and for >21 days by 14% of cardiologists. • Arch Mal Coeur Vaiss. 2006 Jan;99(1):61-4.[Acute pericarditis: results of a survey of treatment practices of cardiologists]
Bacterial pericarditis • Rare, but universally fatal if not Tx(abx, +/- surgery), otherwise MR 40% (tamponade, sepsis) • Hx/exam/labs: ↑ fever, short duration (2 to 3/7), ↑HR, dyspnea, ↑CVP, CP, friction rub, and ↑WBC • Source: • 1) spread from an adjacent infection (i.e.pneumonia) • 2) hematogenous spread from a distant site (MC), • 3) direct inoculation of bacteria (trauma or procedure), • 4) spread from an intracardiac source
RF: immunocompromised, chronic dz (i.e.EtOH, rheumatoid), CV surgery, chest trauma • Tx: as per mgnt of sick/septic pts, CCU/ICU • Vanco + cipro (Sanford Guide) • Pericardial tap (urgent) +/-pericardectomy
Pericarditis and HIV + • Can be infectious, non-infective (i.e Rx) and neoplastic (Kaposi’s, lymphoma) • Tx Sx • ECHO to assess for these causes • +/-pericardiocentesis depending on ECHO findings • Steroids contra-indicated unless TB pericarditis
Uremic Pericarditis • Usually seen with ARF/CRF prior to dialysis • Correlates with degree of azotemia • +/- pericardial rub, usu no ECG changes • Tx with dialysis • +/- pericardial drain/pericardectomy if not improving
Auto-Immune Disease • MC with RA, SLE, Scleroderma • Only Tx if Sx (I.e. don’t Tx if only have mild ECG/ECHO findings) • Tx • Optimize auto-immune disease Tx • NSAID’s • Consider steroids for RA
Pericarditis Prognosis • Excellent • 60% of patients have complete recovery within 1 week, 78% have complete recovery within 3 weeks. • Only 3% have a prolonged course with symptoms for more than 3 weeks before complete resolution
Case #2 • A 47M presents to the ED feeling pre-syncopal and extremely SOB. It’s 3:00am. • Recently Dx with pericarditis and had been doing okay until the past 24 hrs • Patient appears moribund • VS: sBP 75, sats 85%, obvious resp distress • Cardiac: unable to hear his HS, JVP at his jaw • What do you think is going on?
Physical Exam • What is Beck’s triad? • What is the pathophysiology of pulsus paradoxus? • How do you check for it? • How much pericardial fluid
Beck’s Triad
Management of Tamponade? • Temporizing measures? • Non-invasive? • Invasive? • Definitive tx • Surgical or pericardial drain
Complications of Pericarditis • Pericardial Effusion (unsure of IR, but likely <5% for moderate – severe) • Constrictive Pericarditis • Recurrence (15-30%)
Disposition of Pericarditis • Most can be sent home • Clear d/c instructions: return if Sx not improving within next few days, SOB, feeling generally unwell • Admission • Intractable pain • Peri-myocarditis: ↑trop – risk of arrhythmia • Moderate-severe effusion or Tamponade • To r/o other Dx (ischemia, PE)
Case #3 • Myocarditis