Download

1 / 27
290 likes | 467 Views
HbA1C and DM control. By Ri 陳信豪. Introduction. microvascular complications in type 1 diabetes --slowed by treating hyperglycemia increased use of intensive insulin regimens to attain strict glycemic control

E N D
HbA1C and DM control By Ri 陳信豪
Introduction • microvascular complications in type 1 diabetes --slowed by treating hyperglycemia increased use of intensive insulin regimens to attain strict glycemic control • The efficacy of these regimens requires an accurate method to estimate
a given mean blood glucose value associated with different mean glycemic excursions and mean daily differences
Estimation of mean blood glucose by A1C • glucose can attach to many proteins via a nonenzymatic, posttranslational process • (1)A reversible reaction leads to the formation of an aldimine • (2)followed by an Amadori rearrangement to form an irreversible ketoamine.
Glycated hemoglobin • most widely used clinical test measurement of blood glycated hemoglobin (also called hemoglobin A1C, glycohemoglobin, and glycosylated hemoglobin [HbA1c]). • the average amount of A1C changes in a dynamic way reflects the mean blood glucose concentration over the previous six to eight weeks. Nathan, DM, Singer, DE, Hurxthal, K. Goodson, JD. The clinical information value of the glycosylated hemoglobin assay. N Engl J Med 1984; 310:341.
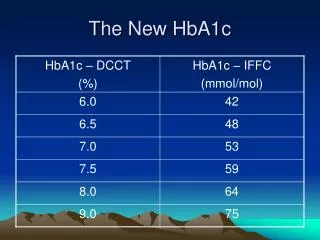
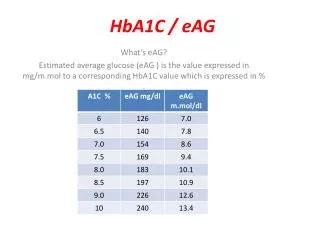
Diabetes Control and Complications Trial (DCCT) • mean blood glucose concentrations from seven measurements a day (before and 90 minutes after each meals, and before bedtime) compared with A1C values in 278 patients with type 1 DM • A strong correlation A1C value of 7 percent --150 mg/dL A1C value of 9 percent --210 mg/dL
Factors causing misleading results • A1C values influenced by red cell survival. (1) falsely high values -- low red cell turnover--disproportionate number of older red cells ex: iron, vitamin B12, or folate deficiency anemia. (2) falsely low values -- rapid red cell turnover – greater younger red cells ex: hemolysis , treated for iron, vitamin B12, or folate deficiency Panzer, S, Kronik, G, Lechner, K, et al. Glycosylated hemoglobins (GHb): An index of red cell survival. Blood 1982; 59:1348.
Fructosamine • nonenzymatic glycation formation of advanced glycosylation end products direct role in the development of diabetic microvascular complications • good correlation between serum fructosamine and A1C values • variation for fructosamine higher than that for A1C • serum fructosamine values reflect mean blood glucose values over a much shorter period of time (one to two weeks).
About type 1 DM--Introduction • nephropathy and retinopathy --more likely to occur in patients with poorer glycemic control • The risk is highest if HbA1c value above 12% Barzilay, J, Warram, JH, Bak, M, et al. Predisposition to hypertension: risk factor for nephropathy and hypertension in IDDM. Kidney Int 1992; 41:723. *The severity of hyperglycemia correlated with recurrent diabetic nephropathy in patients who have received a renal transplant Mauer, SM, Goetz, FC, McHugh, LE, et al. Long-term study of normal kidneys transplanted into patients with type I diabetes. Diabetes 1989; 38:516.
Prospective Diabetes Control and Complications Trial (DCCT) • mean A1C values during the nine-year study 7.2 percent with intensive therapy-- 155 mg/dL 9.1 percent with conventional therapy--235 mg/dL • The DCCT provided conclusive evidence strict glycemic control a) delay the onset of microvascular complications (primary prevention) b) low the rate of progression of already present complications (secondary intervention)
Pathogenesis • 1. Advanced glycosylation end products (AGE) – a) tissue accumulation of AGEs-- crosslinking with collagen-- renal and microvascular complications b) modify LDL-- less cleared by LDL receptors -- hyperlipidemia commonly present in diabetic patients • 2. Sorbitol — a) accumulation within the cells --rise intracellular osmolality and decrease intracellular myoinositol-- interfere with cell metabolism b) major contribution of sorbitol --the cataract formation induced by hyperglycemiaLee, AY, Chung, SK, Chung, SS. Demonstration that polyol accumulation is responsible for diabetic cataract by the use of transgenic mice expressing the aldose reductase gene in the lens. Proc Natl Acad Sci U S A 1995; 92:2780.
Retinopathy • major end-point in many of the prospective diabetes trials because it is the most common microvascular complications • the incidence of new retinopathy 12 % in the intensive therapy group 54 %in the conventional therapy group. • progressive retinopathy -- uncommon at A1C values below 7 %
*the risk of severe hypoglycemic episodes was also continuously, but inversely, related to glycemic control*ranging from approximately 105 to 25 episodes per 100 patient-years at mean A1C values of 5.5 and 10.5 percent, respectively
Established retinopathy • intensive insulin therapy -- slow the rate of progression of mild to moderate retinopathy. • The incidence of worsening retinopathy in intensively treated patients -- higher than in those receiving conventional therapy at one year (7.4 versus 3 percent) but much lower at nine years (25 versus 53 percent).
Intensive insulin therapy for 6.5 years during the DCCT reduced the risk of retinopathy over the next seven years despite an increase in A1C values. Effect of intensive therapy on the microvascular complications of type 1 diabetes mellitus. AMA 2002; 287:2563.
Nephropathy • DCCT included many patients with no detectable microalbuminuria at baseline. After 6.5 years of study, the prevalence of new microalbuminuria -- much lower with intensive therapy-- 16% versus 27 % The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;. * the benefits of intensive therapy for primary prevention of nephropathy persist for a number of years
*strict glycemic control with intensive insulin therapy-- not slow the rate of progressive renal injury once overt proteinuria developed (albumin excretion greater than 300 mg/day). • At late stage--often marked glomerulosclerosis. Only antihypertensive therapy (preferably with ACEI) and perhaps dietary protein restriction – --slow the rate of progressive disease or reverse established lesions.
Neuropathy • Intensive insulin therapy -- reduced the incidence of abnormal nerve conduction associated with improvement in nerve conduction velocity • The Oslo study -- graded effect of hyperglycemia on disease progression each 1% rise in A1C values associated with 1.3 m/sec slowing of nerve conduction at eight yearsAmthor, KF, Dahl-Jorgensen, K, Berg, TJ, et al. The effect of 8 years of strict glycaemic control on peripheral nerve function in IDDM patients: The Oslo Study. Diabetologia 1994; 37:579
Macrovascular disease • nonsignificant trend toward fewer cardiovascular events with intensive therapy (3.2 versus 5.4 percent, p = 0.08) • The intensive insulin therapy group -- lower serum LDL but some weight gain due to the increase in insulin administration • Mean progression of intima-media thickness of carotid artery significantly less in intensive therapy compared with conventional therapy (0.032 versus 0.046 mm). not known about reduction in cardiovascular disease-related events.
About type 2 diabetes mellitus- The United Kingdom Prospective Diabetes Study (UKPDS) • strict control also reduced risk of microvascular disease in type 2 DM • Over 10 years, the average A1C value was 7.0 percent in the intensive-therapy group compared with 7.9 percent in the conventional-therapy group
*Most of the risk reduction in the intensive therapy group --due to 25 % risk reduction in microvascular disease (P = 0.001) *There was no reduction in macrovascular disease. • The benefits of intensive therapy -independent of the type of treatment administered. • The reduction in microvascular complications in intensive therapy -- a smaller magnitude than in patients with type 1 diabetes in the DCCT
Macrovascular disease in type 2DM • Conflicting data on the importance of glycemic control on the development of macrovascular disease in type 2 DM • To date, no randomized clinical trial has convincingly demonstrated a beneficial effect of intensive therapy on macrovascular outcomes in type 2 DM • The most effective approach for prevention of both micro- and macrovascular complications multifactorial risk factor reduction (glycemic control, stopping smoking, aggressive blood pressure control, treatment of dyslipidemia, and daily aspirin).
Summary(1-1)-Type 1 DM • strict glycemic control-- before irreversible end-organ damage -- reduces the incidence of microvascular disease and neurologic dysfunction in type 1 diabetes. • From a renal viewpoint, this regimen -- beneficial in all patients except overt proteinuria in whom strict blood pressure control with an ACE inhibitor appears to be more important • Beginning intensive therapy as early as possible after the diagnosis and measure HbA1C three to six months.
Summary(1-2)-Type 1 DM • In general, we aim for a A1C value of approximately 7% in optimally compliant and non-pregnant patients. • Achieve A1C <7 % should only be considered a) hypoglycemia is not an important problem b) during pregnancy in type 1 and type 2 diabetic women, since the demonstrated benefits to the fetus and neonate drive the therapeutic goals.
Summary(2-1)-Type 2 DM • Outcomes improved for every 1% drop in A1C and there was no threshold effect, a reasonable goal of therapy might be a A1C value of 7.0 % for most patients • The ADA also recommends a target of less than 7.0 % for most patients, while the American Academy of Clinical Endocrinologists (AACE) and the European Association for the Study of Diabetes (EASD) both recommend a target of A1C less than 6.5 %
Summary(2-1)-Type 2 DM • From a practical standpoint, we are limited from pushing A1C lower due to increased risk of hypoglycemia, weight gain, and the cost of using multiple drugs to achieve the goal • Vigorous cardiac risk reduction (smoking cessation, aspirin, blood pressure, reduction in serum lipids, diet, exercise, and, in high-risk patients, an ACEI) should be a top priority for all patients with type 2 diabetes • The HbA1C goal should be set somewhat higher for older patients and those with a limited life expectancy.
樂 新 快 年 萬 事 如 意