Download
1 / 29
300 likes | 665 Views
Hospital Care of Patients With Sleep Apnea. Steve Marks, DO FCCP FAASM Medical Director Arete Sleep Health Director Critical Care: Banner Gateway Medical Center. Sleep Apnea Definitions. Central apnea Lack of airflow and lack of Inspiratory effort for 10 seconds. Obstructive apnea

E N D
Hospital Care of Patients With Sleep Apnea Steve Marks, DO FCCP FAASM Medical Director Arete Sleep Health Director Critical Care: Banner Gateway Medical Center
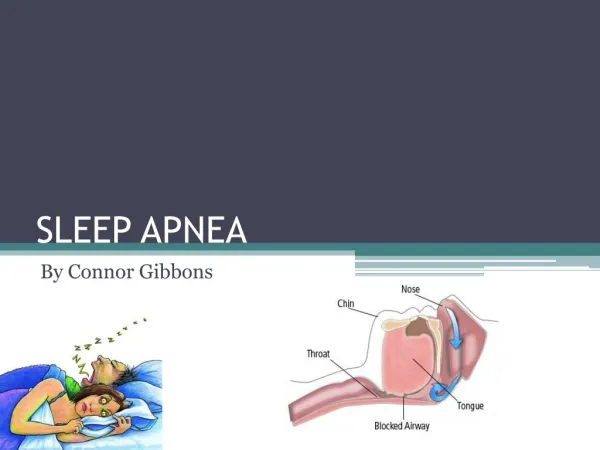
Sleep Apnea Definitions • Central apnea • Lack of airflow and lack of Inspiratory effort for 10 seconds. • Obstructive apnea • Lack of airflow associated with continued or increased respiratory effort for 10 seconds. • Hypopnea • Decrease in airflow of > 30% associated with > 4% decrease in saturation with a duration of 10 seconds. • RERA • Does not meet criteria for apnea or hypopnea. • Increasing respiratory effort over 10 seconds.
Characteristics of OSA • Snoring & observed apneas. • Hypersomnolence. • AM Dry mouth, headache. • Insomnia. • Narrowed airway • Large neck • > 17” male • > 15” female • Obesity • Malocclusion • Retrognathia.
Pathophysiology of Sleep Apnea Awake: Small airway + neuromuscular compensation Sleep Onset Hyperventilate: connect hypoxia & hypercapnia Loss of neuromuscular compensation + Decreased pharyngeal muscle activity Airway opens Pharyngeal muscle activity restored Airway collapses Arousal from sleep Apnea Increased ventilatory effort Hypoxia & Hypercapnia
Home CPAP Less obtrusive than in hospital CPAP. Large variety of mask styles and sizes.
Mechanism of Hypoxemia During REM Sleep in COPD • Decreased FRC. • Decreased oxygen reserve. • Hypoventilation. • REM sleep-associated inhibition of respiratory muscles. • Decreased chemo sensitivity to PCO2 and PO2. • Altered V/Q relations. • Position of baseline saturation on oxygen-hemoglobin desaturation curve.
Renal failure altered sleep in Uremia. Medications. Liver failure. Encephalopathy. Disruption to sleep continuity. Environmental disturbances. Noise, light, nocturnal activity, loss of schedule. Relaxed upper airway. Rebound REM sleep. Rebound slow wave sleep. Confusion. Sleep in Hospitalized patients
Treatment Options • Minimize medications that relax airway. • Minimize sleep disruption which lead to sleep rebound. • Supplemental oxygen. • Home CPAP/BiPAP. • Empiric CPAP/BiPAP. • Auto Titrating CPAP. • Auto Servo Ventilation.
Sleep in the ICU • Increased arousals and decreased sleep efficiency. • Increased sleep during day. • Increase lighter stages of sleep. • Decrease SWS and REM. • Included typical sedation (benzodiazepines and opioids) • Excluded patients who received general anesthetic. Cooper et al; Cest/117/3/2000
Comorbidities • Influence OSA • Psychiatric medications • Suppress REM sleep. • Relax dilator muscles of airway and tongue. • Pain medications • Relax dilator muscles of airway and tongue. • Narcotics may cause central apneas. • Anesthetics • Relax dilator muscles of airway and tongue. • REM rebound.
Respiratory Failure • Patients have increased risk of OSA: • Sedating effects of medications. • Respiratory depression. • Relaxation of genioglossus, and pharygeal dilator muscles. • Upper airway edema. • Decreased pulmonary reserve: • Decreased FRC. • Baseline hypoxemia. • REM rebound following sleep deprivation. • Limited ability to change position.
Respiratory FailureTreatment Strategy • Minimize systemic narcotics and hypnotics. • Adherence to scales for assessment and treatment of sedation, pain, and delirium. • Use of appropriate medications for delirium. • Use of epidural and local analgesia. • Semi recumbent posture. • Incentive spirometry/IPPB. • Minimize sleep disruption. • Noninvasive ventilation. • Positive pressure devices.
Sleep in COPD • Increased sleep latency. • Shortned total sleep time. • Increased arousals. • Increase in lighter stages of sleep. • Insomnia & EDS worse with increasing respiratory symptoms.
Nocturnal Peak Flow • Drop in catecholamines. • Drop in cortisol. • Coincides with highest percentage of REM sleep during the night.
Overlap Syndrome • Coexistence of COPD and OSA. • Exacerbation of hypoxemia during sleep with similar characteristics of AHI. • Lower waking PO2 and Higher PCO2. • Increased pulmonary artery pressures. • Blunted CO2 response during sleep. • Lower 5 years survival.
COPD • Inhaled cholinergics have been shown to improve mean nocturnal SaO2, perceived sleep quality, and increase REM time. • Oral Theophylline shown to improve nocturnal oxygen saturation and AM peak flow. • Noninvasive positive pressure ventilation improves acute exacerbation of COPD. • Avoid medications that relax airway or depress respiration. • Inspiratory muscle training in long term can improve nocturnal oygenation. DC plan to include pulmonary rehab.
COPDTreatment Options for OSA • Optimize medications around known dip in nocturnal peak flow. • Minimize entities that exacerbate airways obstruction: • Control reflux. • Avoid cool air. Humidify oxygen. • Identify and avoid allergens: Latex. • Positive pressure. • Avoid sedating medications and hypnotics.
Long Term Risk Hypertension. LVH. RVH. Direct. Secondary to PAH. Arrhythmia. Increased atherosclerosis. Acute Risk in Hospital Pulmonary Edema. Arrhythmia. Extension of MI. Increase inflammatory milieu. Respiratory failure. Cardiac Risk Related to OSA
Congestive Heart Failure • Supplemental oxygen. • CPAP. • BiPAP. • Autotitrating positive pressure. • Telemetry monitoring. • Minimize narcotics and benzodiazepines. • Treat nasal obstruction.
Central Sleep Apnea • Adaptive Servo Ventilation. • BiPAP with backup rate. • CPAP. • Oxygen. • Medications: • Theophylline. • Acetazolamide.
Ischemic Cardiac Disease • Tx underlying OSA. • Positive pressure. • Minimize narcotics and benzodiazepines. • Supplemental oxygen.
Preoperative Evaluation • Medical record review. • Patient or family interview. • Physical examination. • Review of sleep studies.
Preoperative Recommendations • Initiate CPAP. • Consider NIPPV. • Wt loss if feasible. • Pts with history of sleep surgery presumed at risk until polysomnogram demonstrates otherwise. • Evaluate for local or regional anesthesia and analgesia.
ASA Interoperative Recommendations • Verification of reversal of neuromuscular blockade prior to extubation. • Extubation when fully awake. • General anesthesia with a secure airway preferable to deep sedation for superficial procedures or endoscopy in a patient at risk.
Post Operative Recommendations • CPAP. Start in PACU. • Monitoring; continuous pulse ox, heart rate, and rhythm. • Minimize systemic analgesia and IV patient controlled analgesia. • Use regional analgesia (local or epidural) whenever possible. • Be aware of REM rebound. • Avoid excessive tightness of abdominal binders. • Encourage incentive spirometer. • May require prolonged monitoring.
Post Discharge Recommendations • CPAP. • Polysomnogram when indicated. • Education. • Ensure followup with primary care physician. • Communication with sleep lab.
General Recomendations • Education of RT’s, RN’s, to OSA. • CPAP. • Autotitrating and Bilevel devices. • Pathophysiology of OSA. • Recognition of OSA. • RT’s need to have expertise in mask fitting. • A variety of masks need to be available. • Minimize narcotic and benzodiazepine medications.