Download
1 / 21
220 likes | 625 Views
Nutrition Therapy for Liver & Gallbladder Diseases. Chapter 20. Functions of Liver & Gallbladder. Liver—most active organ in body Receives & processes nutrients absorbed by small intestine Makes bile for fat emulsification Synthesizes most proteins circulating in plasma

E N D
Nutrition Therapy for Liver & Gallbladder Diseases Chapter 20 Nutrition & Diet Therapy, 7th Edition
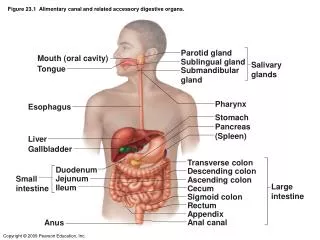
Functions of Liver & Gallbladder • Liver—most active organ in body • Receives & processes nutrients absorbed by small intestine • Makes bile for fat emulsification • Synthesizes most proteins circulating in plasma • Detoxifies drugs & alcohols • Processes excess nitrogen for excretion as urea • Liver damage or disease can profoundly affect health & nutritional status Nutrition & Diet Therapy, 7th Edition
I. Fatty Liver & Hepatitis • Most common of liver disorders • Usually mild & reversible, but can progress to serious illness & liver damage Nutrition & Diet Therapy, 7th Edition
Accumulation of fat in liver tissue; represents imbalance between fat synthesized from the blood & the amount exported to the blood via VLDL Causes are unclear, but associated with: Alcoholic liver disease Result of exposure to drugs & toxic materials Associated with obesity, diabetes mellitus, diseases of malnutrition May follow gastrointestinal bypass surgery or long-term TPN Consequences Liver enlargement (hepatomegaly), inflammation, fatigue Abnormal levels of liver enzymes Increased levels of triglycerides, cholesterol, glucose Liver damage & failure Treatment Elimination of factors causing it Weight reduction Control of blood glucose levels Fatty Liver Nutrition & Diet Therapy, 7th Edition
Inflammation of liver, resulting from damage to liver tissue Cause often infection with specific viruses (A, B, C) Usual transmission Blood contact with infected persons Ingestion of contaminated food or water Excessive alcohol intake or exposure to certain drugs & toxic chemicals Symptoms Effects depend on cause & severity of disease Fatigue Nausea, anorexia Pain in liver area Liver enlargement Jaundice Fever Headache, muscle weakness Skin rashes Elevation of liver enzymes (ALT, AST) Hepatitis Nutrition & Diet Therapy, 7th Edition
Hepatitis • Treatment • Supportive care; bed rest & appropriate diet • Avoidance of substances that aggravate liver (alcohol, drugs or dietary supplements that cause liver damage-chaparral, germander, ma huang, saw palmetto and jin bu huan) • Hepatitis A usually resolves without medications • Hepatitis B & hepatitis C infections may require antiviral agents • Nonviral forms: treated with anti-inflammatory & immunosuppressant drugs • Nutrition therapy • May require high-kcalorie, high-protein diet to replenish nutrient stores • Liquid supplements may improve nutrient intakes • Small, frequent meals easier to tolerate for patients with anorexia or GI discomfort • Fluid & electrolyte replacement necessary in case of vomiting • Sodium & fat restriction may be recommended Nutrition & Diet Therapy, 7th Edition
End-stage condition resulting from chronic liver disease Gradual destruction of liver tissue, leading to scarring Progressive disease results in increased scarring, few areas of healthy tissue Impairs liver function & can lead to liver failure Causes Alcohol abuse & hepatitis C infection most common causes Chronic hepatitis Drug-induced Inherited disorders Bile duct blockages Consequences Initial disease: mild or asymptomatic, fatigue, weakness, anorexia, weight loss Later disease: decline in liver function, anemia, impaired blood clotting, increased susceptibility to infection, jaundice, fat malabsorption Advanced disease: disruption of kidney & lung function Altered liver enzymes, bilirubin levels Lowered albumin levels, extended clotting times Elevated blood ammonia levels II. Cirrhosis Nutrition & Diet Therapy, 7th Edition
Consequences (con’t) Portal hypertension Scarred tissue of cirrhotic liver impairs blood flow through liver Resistance to blood flow increases pressure in portal vein: portal hypertension Collaterals & gastroesophageal varices Collateral circulation-smaller blood vessels enlarge to allow alternative pathway for blood flow because (in GI tract & near abdominal wall) As a result, varices form (collaterals become enlarged & engorged with blood) Ruptured esophageal or gastric varices can result in massive bleeding, often fatal Ascites Accumulation of fluid in the abdominal cavity; indicates critical stage of liver damage Thought to be consequence of portal hypertension, reduced albumin synthesis & altered kidney function Hepatic encephalopathy: characterized by abnormal neurological functioning Changes in personality, mental abilities & motor function Amnesia, seizures Hepatic coma Elevated blood ammonia levels Malnutrition & wasting Cirrhosis Nutrition & Diet Therapy, 7th Edition
Treatment of Cirrhosis • Individualized according to disease severity & complications • Supportive care • Appropriate diet • Avoidance of liver toxins • Abstinence from alcohol • Drug therapy • Medications for portal hypertension, varices • Diuretics • Appetite stimulants • Medications to reduce or control blood ammonia levels • Nutrition therapy • Customized for each patient’s needs • Avoidance of substances that can cause further liver damage • Enteral & Parenteral nutrition support as indicated Nutrition & Diet Therapy, 7th Edition
III. Liver Transplantation • Liver failure (resulting from acute or chronic liver disease) may require transplantation as only treatment option • Most common result of hepatitis C infection or alcoholic liver disease • Nutrition status of transplant patients • Usually associated with malnutrition (common with advanced liver disease) • Correction of malnutrition prior to surgery can help speed recovery • Associated deficiencies: vitamins B6, B12, C, thiamin, niacin, folate, fat-soluble vitamins, calcium, magnesium, phosphorus, potassium, zinc Nutrition & Diet Therapy, 7th Edition
Liver Transplantation • Post-transplantation concerns • Immediate concerns: organ rejection & infection • Immunosuppressive drugs reduce immune response that causes rejection, but increase risk of infection • Effects of immunosuppressant drugs on nutrition • GI side effects (nausea, vomiting, diarrhea, abdominal pain, mouth sores) • Alteration in appetite & taste perception • Hyperglycemia, diabetes • Fluid & electrolyte imbalances • Hypertension, hyperlipidemia, protein catabolism, increased osteoporosis risk • Increased protein & energy requirements after transplantation due to stress of surgery; includes snacks and enteral supplements. • Vitamin & mineral supplementation • Food safety concerns to reduce risk of food-borne illnesses Nutrition & Diet Therapy, 7th Edition
Gallstones (cholelithiasis) Gallbladder stores the bile made by the liver Disorders of gall bladder & bile ducts result in formation of gallstones Results from excessive concentration & crystallization Two Types 1. Cholesterol gallstones: majority of cases of gallstones; composed primarily of cholesterol; precipitation of cholesterol out of solution eventually forms stones 2. Pigment gallstones: composed mainly of calcium salt of bilirubin; often result of bacterial infection IV. Gallbladder Disease Bile: solution of bile salts, cholesterol, proteins, phospholipids & bilirubin Nutrition & Diet Therapy, 7th Edition
Consequences of gallstones Many asymptomatic Other symptoms—usually occur when gallstones block cystic duct Steady & severe pain Nausea, vomiting, bloating Symptoms mainly occur after meals, especially fatty foods Complications Cholecystitis Peritonitis Blockage of common bile duct Infection Risk factors for gallstones Ethnicity Age & gender Pregnancy Obesity & weight loss Other risk factors Long-term TPN Medications High TG levels Treatment Low fat diet Cholecystectomy Non-surgical Capsule urso-deoxycholic acid (”cholesterol production; used on small stones) Shock-wave lithotripsy (used on few and larger stones) Gallbladder Disease Nutrition & Diet Therapy, 7th Edition
Nutrition in Practice—Alcohol in Health & Disease • Excessive alcohol consumption is primary cause of liver disease • Can result in toxicity to other organs, including brain, GI tract, pancreas • Moderate use, however, shown to reduce deaths from coronary heart disease in middle-aged & older adults • Current dietary guidelines (Dietary Guidelines for Americans 2005) • Adults should limit intake to 1 drink/day (women) to 2 drinks/day (men) • Avoidance of all alcohol: pregnant & lactating women, women who may become pregnant, children & adolescents, individuals who are taking medications that may interact with alcohol, individuals who are unable to voluntarily restrict intake Nutrition & Diet Therapy, 7th Edition
Alcohol in the body Source of food energy (providing 7 kcalories per gram) Quickly absorbed in stomach & small intestine; passes readily into body cells Liver is site of most alcohol metabolism Metabolism in liver takes priority over metabolism of other substances Interferes with metabolism of other substances Suppresses storage of glycogen & availability of glucose between meals, increasing risk of hypoglycemia Suppresses breakdown of fat for energy, increasing VLDL Inhibits protein synthesis Cellular toxicity Alcohol alters structure of cell membranes, interferes with actions of cell membrane proteins Under certain conditions, exposure to alcohol can induce cell death Effects on brain function Acts as central nervous system depressant Causing sedation Slowing reaction times Relieving anxiety Extremely high blood alcohol levels can lead to coma & death Chronic heavy drinking can lead to neurological damage Nutrition & Diet Therapy, 7th Edition
Effects of excessive alcohol consumption on nutrition status—nutrient deficiencies • High kcalorie content displaces other energy sources, including essential nutrients • Widespread malabsorption occurs as result of damage to GI mucosa • Interferes with body processing of nutrients • Increased destruction of vitamin A • Reduction of thiamin (vit. B1) absorption & activation • Reduction of folate absorption • Disruptive effect on metabolism of medication Nutrition & Diet Therapy, 7th Edition