Download
1 / 27
290 likes | 940 Views
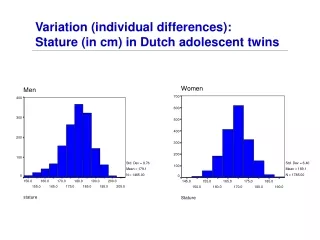
Short Stature. : Done by Asim .Q. Makhdom. Def: . Height less than 3 rd percentile for age and sex Percentile SDS 3rd 1.9 2,5 th 2

E N D
ShortStature :Done by Asim .Q. Makhdom
Def: Height less than 3 rd percentile for age and sex Percentile SDS 3rd 1.9 2,5th 2 1st 3
Growth velocity • The faster growth occur in UTERINE LIFE • Peak around 4th month of gestation • Slow down till birth • The 2ed acceleration takes place at PUBERTY
Growth velocity (cont) • Girls have their pack growth velocity (9cm/y)during early puberty and before menarche • Boys have their pack (10.3cm/y)during mid puberty
DD 1.Familial 2.IUGR 3.Constitutional delay in growth 4.Endocrine 5.Nutretional 6. Syndromes 7.dispropotion. 8.psycological
Growth depend : • Genetic factors: single gene disorder Vs polygenic mid parental high =target high boy(father +mother+13)/2= +_ 8,5 cm Girl(father+mother-13)/2=+-8,5 cm
Endocrine disorders • GH deficiency • Hypothyroidism • Increase cortisone • DM • DI • Emotional deprivation(psychosocial dwarfism)
Malnutrition(35%) • Kwashiorkor and marasmus • Iron deficiency • Zink deficiency • Rickets
Skeletal diseases • Osteogenesis imperfecta • Osteochondroplasia • Achondroplasia
Chronic diseases(20%) • Cardiac :eg:CHD • Plumonary:CF,asthma,TB • Renal : RTA,CRF • GIT : IBD • Hepatic : liver cirrhosis • CNS : CP
Primordial disorders • Turner”s syndrom • Noonan syndrom • Autosomal trisomy: eg: Down's syndrome
History • A careful and detailed history is an important part when assessing growth. Details of pregnancy, maternal healthand birth should be addressed. In addition to inquiring about birth weight and length, the occurrence of specific prenatal, prenatal, or postnatal complications should be questioned. For example, at birth a hypoxic insult may cause hypothalamic hypopituitarism, and neonatal hypoglycaemia may imply growth hormone deficiency. Early health, past medical history and treatment, and age of recognition of short stature are important questions to ask. For example, treatment of asthma with chronic systemic or inhaled glucocorticoids can cause poor growth
Obtaining old growth records with data on height and weight is pertinent when assessing growth. • (assessment over six months to one year) will differentiate normality from abnormality. • The height of both parents, age of onset of puberty, nutritional status, and social background are also relevant. • A family history of pubertal delay is often found in children with constitutional short stature. • Finally, genetic potential can be predicted on the basis of parental heights, and it is the midparental height which provides information necessary to determine if the child's height is appropriate for his or her family
it is useful to define whether short stature is proportionate or disproportionate. • The sitting height plotted against total height on an appropriate chart will help in the differential diagnosis of short stature (proportionate versus disproportionate). • In addition, the ratio of upper to lower body segment is most often disproportionate in patients with primary bone disorders. • On the other hand, this ratio is normal (proportionate) in patients with chronic diseases, both endocrine and non-endocrine. • The lower segment is the distance between the top of the symphysis pubis and the floor when the patient is standing; the upper segment is calculated by subtracting the lower segment from the standing height.
Physical examination • should include pubertal staging and documentation of testicular volume using a Prader orchidometer. • Both visual acuity and visual fields ought to be checked, bearing in mind the possibility of a hypothalamic pituitary lesion. • Finally, general physical examination may disclose features of recognised syndromes (for example, Turner's syndrome) or chronic disorders.
Wight • Height • Bone age • Disproportions
Investigations • Bone age • TFT • Karytype in girls • CBC and ESR • U&E • Urine analysis and stool analysis • GH test
Summary a good history and physical examination identify most pathological causes of short stature Focus on looking for signs of intracranial pathology, hormones deficiency, chronic illness and GIT symptoms. Relate the child’s height to the parents' heights. Identify any emotional and social consequence of being short.