Download
1 / 23
250 likes | 476 Views
Presented by the Region 2 group: Mari Garza-Facilitator Yvette Bowerrman Silvia Gonzalez Lori Irvine Susan Little Jody Harris DeLeon. Glaucoma . Glaucoma.

E N D
Presented by the Region 2 group: Mari Garza-Facilitator Yvette Bowerrman Silvia Gonzalez Lori Irvine Susan Little Jody Harris DeLeon Glaucoma
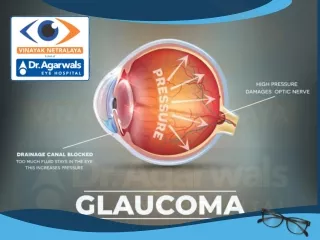
Glaucoma • Is a complicated group of diseases in which the intraocular pressure (IOP) of the eye is abnormally elevated. This abnormally high pressure results in optic nerve damage and eventually blindness. • Glaucoma is the second leading cause of blindness. • Sometimes it is referred to as the “silent thief of sight”. • Glaucoma onset can either be a steady loss of sight or immediate due to trauma to the eye.
Types of Glaucoma • There are several types of Glaucoma Primary Open-Angle Glaucoma Angle-Closure Glaucoma Normal-Tension Glaucoma Secondary Glaucoma Childhood Glaucoma
Primary Open-Angle Glaucoma • Most common type of glaucoma. It affects at least 3 million Americans annually. • Occurs when the eye’s drainage canals congested over time, and the aqueous fluid cannot drain appropriately, causing the intraocular pressure of the eye to become abnormally high. • There are no early warning signs or symptoms. Most people find that they have this condition during a routine tonometry (the puff test) test. • If not treated Open-Angle Glaucoma will result in a gradual loss of vision.
Angle-Closure Glaucoma • Also known as “Acute Glaucoma” or “Narrow-Angle Glaucoma”. • This type of Glaucoma occurs when the drainage canals are blocked or covered by the edge of the Iris because it is not as wide or open as it should be. • Occurs most often when the pupil dilates to quickly or to much. This can happen when entering a dark room. • Symptoms include: headache, eye pain, nausea, rainbows around lights at night, and very blurred vision. • Treatment includes surgery to unblock the drainage canals by removing the outer edge of the iris. Surgery is usually successful and long lasting. However, it is recommend that patients continue with their regular eye doctor visits.
Normal-Tension Glaucoma • Also called “low tension” or “normal-pressure glaucoma” • This form of Glaucoma in which the optic nerve is damaged without the IOP being outside the “normal range” of 10-20 mm Hg. • Causes for this form of Glaucoma are still unknown. • People who are at risk for this type of Glaucoma: are ones with a family history of this type of glaucoma, people of Japanese ancestry, and people with a history of systematic heart disease such as an “irregular heart rhythm” • Diagnosis is done by looking for signs of optic nerve damage. This can be done one of two ways:
Normal-Tension Glaucoma (cont) • First procedure is to use an ophthalmoscope. Your Optometrist or Ophthalmologist will hold the scope up close to your eye, and examine the shape and color of the optic nerve. This procedure is normally done during a routine exam and in a dark room. • Second procedure is the Visual Field Test. This test creates a map of your complete field of vision. The doctor uses this “map” to check for any scotoma that is caused by damage to the optic nerve. • Symptoms include: slight changes in a person’s visual field that might occur near the center or to the edge of the visual field. • Treatment includes: medications, laser treatments and in some cases conventional surgery
Secondary Glaucoma's • Secondary Glaucoma's occur when another disease causes or contributes to a rise in IOP. • Secondary Glaucoma's can also occurs during a eye injury, inflammation, tumor, or in advanced cases of cataract or diabetes • There have been cases where drugs, such as steroids, causing a mild or severe form of secondary glaucoma. • There are 6 types of Secondary Glaucoma: pigmentary glaucoma, pseudoexfoliative glaucoma, traumatic glaucoma, neovascular glaucoma, irido corneal endothelial syndrome (ICE), and congenital glaucoma (childhood glaucoma).
Secondary Glaucoma (cont) • Pigmentary Glaucoma occurs when the pigment granules in the iris break into the aqueous humor and flow toward the drainage canals of the eye and clog them. Treatment is medication, laser or conventional surgery. • Pseudoexfoliative Glaucoma occurs when a dandruff like substance peels off of the outer layer of the lens. This substance collects in the angle between the cornea and the iris, causing the drainage system to clog and the IOP to rise. This type of Glaucoma occurs most often with people of Scandinavian descent. Treatment is medication or surgery.
Secondary Glaucoma (cont) • Traumatic Glaucoma occurs immediately after a blunt, bruising or penetrating injury to the eye. It can also occur years later after this injury has healed. • Conditions such as severe myopia, previous injury or infection or prior surgery can make the eye more vulnerable to this type of glaucoma. • Treatment includes medication, filtration surgery, laser surgery, and tube shunt devices.
Secondary Glaucoma (cont) • Neovascular Glaucoma occurs when there is an abnormal formation of new blood vessels on the iris and drainage canals. • Neovascular Glaucoma is always associated with other abnormalities such as diabetes. • The new blood vessels block the ability of the eye to drain fluid from the trabecular meshwork causing the IOP to rise. • Very difficult to treat. Some treatments include treatment for underlying disease, filtration surgery, transscleral diode laser retinopexy, or if needed, a lensectomy.
Secondary Glaucoma (cont) • ICE (Irido Corneal Endothelial Syndrome) is rare and occurs in one eye, rather than both. Corneal cells spread over the eye’s drainage canals and across the iris, causing canal blockage and an increase in the IOP. These “cells” form adhesions that bind the iris to the cornea causing more blockage in the drainage canals. Occurs more frequently in “light-skinned” females. Symptoms include: hazy vision when awaken and halo’s around lights. Treatment can include medications and filtration surgery.
Childhood Glaucoma • Refers to the presence of glaucoma in a child. This secondary form of glaucoma occurs in 1 out of 10,000 births in the United States. • Also known as Congenital Glaucoma. • Childhood Glaucoma is diagnosed in either infancy or early childhood. • This Glaucoma is caused by an abnormal intraocular fluid drainage that results in a blocked or defective trabecular meshwork. • Congenital Glaucoma can be contributed to abnormal development during pregnancy or a hereditary genetic defect.
Symptoms of Childhood Glaucoma • Symptoms of Childhood Glaucoma include Epiphora ( impairment of the elimination of tears), blepharospasm ( the involuntary muscle spasm of the eyelid caused by a progressive neurological disorder) • Most common symptoms are excessive tearing, light sensitivity, closure of one or both eyes in the light, cloudy, enlarged cornea ( large eye), vision loss in one or both eyes. • If IOP rapidly increases pain or discomfort may occur as evident by the child becoming irritable, fussy and poor appetite.
Diagnosis of Childhood Glaucoma • Childhood Glaucoma is diagnosed by a completing a full medical history and an eye examination of the child. • The Ophthalmologist will conduct a visual acuity test, a pupil dilation to allow the doctor a close-up view of the retina and optic nerve, a visual field test ( to determine the child’s loss of peripheral vision), and tonometry. • Many children are diagnosed before they are 6 months old. It is very important for early detection to prevent loss of vision.
Treatment of Childhood Glaucoma • If the case is uncomplicated, microsurgery can correct the structural defects of the eye. • Other cases maybe treated with medication and surgery. • Types of surgery may include trabeculotomy, goniotomy, a trabeculectomy, iridotomy, and cyclophotocoagluation. • In trabeculotomy, a outer surgical opening is made in the trabecular meshwork system that establishes a more normal interior chamber angle that allows the aqueous fluid to drain more freely. • A goniotomy creates an inner surgical opening of the trabecular meshwork system to help establish a more normal flow. • A trabeculectomy removes part of the meshwork drainage system to allow fluid to flow normally.
Treatments (cont) • An iridotomy is when a small hole is made through the iris to relieve the IOP. Iridotomy is often with a laser. • A cyclophotocoagulation is often used in cases of severe childhood glaucoma. A laser beam freezes selected parts of the ciliary body to reduce production of the aqueous humor. • Both medications and surgery have been successful with most cases.
Alternative Treatments • Micro puncture • As of 2011 there are 5 states in the Union that allow the use of medicinal marijuana for the treatment/ management of Glaucoma.
Educational Implications of Chilhood Glaucoma • Early intervention is very important in managing childhood glaucoma. Early intervention is designed to assess the child’s needs and create a program that fits that individual. Early intervention will also help the child transition into a preschool or early childhood program at the local school district. • During early intervention, a consult with a teacher of the visually impaired is important so that IEP can be developed to fit that child’s educational needs in the classroom. • It is important during the development of the IEP, that parents consider what works at home for the child. With these adaptations in mind, the TVI can develop more appropriate IEP goals and accommodations for the student and the teacher(s). Parents should make sure that all goals, accommodations and medical history should be written down during the IEP/ARD process.
Educational Implications (cont) • Accommodations that could be considered for classroom use are 1. having the child sit with his/her back to a bright light to avoid glare 2. Simple background for assignments. 3. An uncluttered work area 4. Flexible seating if visual props are used during direct instruction. 5. Have the child wear sunglasses or hats during outdoor playtime to reduce glare. 6. Wear protective goggles during physical activities. 7. Use a Closed Circuit Television (CCTV) to enlarge printed material. 8. Use various muted colors of paper and enlarged writing for assignments. 9. Most importantly, parents need to develop a support network that includes family, friends and various glaucoma support agencies.
Case Study • Student: JV • Aransas Pass ISD • Presented by Lori Irvine
Resources Children’s Hospital Boston(2011)”Glaucoma(disease information) "Retrieved July 27, 2011 from http://www.childrenshospital.org/az/site961/mainpageS961POhtml. Glaucoma Research Foundation.(2011)”What is Glaucoma?” Retrieved July 27, 2011 from http://www.glaucoma.org. Griggs, Paul, B.,M.D. and PubMed Health ( August 6,2009) “Glaucoma”. Retrieved July 27, 2011 from http://www.ncbi.nlm.nih.gov/pubmedhealth/pmh0002587. Mayo Clinic Staff. (1998-2011). “Glaucoma”. Retrieved July 27,2011 from http://mayoclinic.com/health/glaucoma/DS00283. Piedmont Hospital.(2011)”Childhood Glaucoma” Retrieved July 27, 2011 from http://www.piedmonthospital.org/diw/content/asp?pageid=P01206. Willis Eyes(2004-2009)”Childhood Glaucoma”. Retrieved July 27,2011 from http://www.williseye.org/patients/services/glaucoma/childhood/index.html.
Individual/Family Support GroupInformation • See brochure and Support Group List.