Download
1 / 15
160 likes | 365 Views
Dr. Joshua Kimani University of Manitoba & Nairobi Research Group. Female Sex Workers Cohorts . HIV/AIDS in Kenya- Contextual issues. Estimated Population- 35 m (GDP – USD 530) 1.4 m Kenyans estimated to be living with HIV National HIV Prevalence 2003: Kenya Demographic HS- 7%

E N D
Dr. Joshua Kimani University of Manitoba & Nairobi Research Group Female Sex Workers Cohorts
HIV/AIDS in Kenya- Contextual issues • Estimated Population- 35 m (GDP – USD 530) • 1.4 m Kenyans estimated to be living with HIV • National HIV Prevalence 2003: Kenya Demographic HS- 7% -Surveillance 2007- 5.6% • Negative impact on all sectors of the society • 50% to 70% of Medical hospital beds occupancy is linked to HIV (Out of pocket financing being the norm) • Reversed previous health gains: life expectancy 62 to 46 years • About 200000 individuals are currently on ART up from about 10000 in 2004 • With the support from PEPFAR and Global Fund;-Antiretroviral therapy and HIV palliative care became part of the MOH standard of care in 2005
UoM/UoN Research Group- Nairobi, Kenya • Worked closely with female sex workers since 1985 • Initial program started in response to a GUD (Chancroid) outbreak in Nairobi around 1982 • Oldest clinic based at the Majengo slums of Nairobi, while Korogocho and Kibera are the two less known cohorts • The three cohorts -targets low socio-economic Female sex workers • Average of 5 sex partners /day with a high rate of partner change • Marginalized and vulnerable population • All at high risk of HIV transmission and acquisition
Program Goals • Provision of a standardized care package and counseling support that assures prevention of STIs/ HIV • Conducting epidemiological and immuno-biology research studies among the female sex workers • Advocacy for sex worker’s issues • Linkages to programs that offer social support and possible exit strategies
Majengo Sex Workers Cohort • Initial group of female sex workers were mobilized and recruited into the cohort in 1985 • ?Oldest cohort – in Africa • Open cohort with over 3000 participants enrolled to date • Twice yearly resurveys is a unique tradition started in 1985 and maintained today • About 700 on active follow- up during a single resurvey • Contributed a wealth of information on HIV natural history and resistance to date • May provide a natural model of HIV immunity NB: Over 95% of those who need ARVs on medication now
Majengo Cohort: Success factors • Sex workers involvement in programming from the outset • Peer led outreach and cohort cohesion program • Emphasis on ‘informed consent’ at baseline • Basic attitude of service providers assuring confidentiality • Continuous exchange of information through individual, mini and yearly baraza’s • STI screening and management linked to the monthly follow-ups and biannual resurveys • Use of cell phones ‘sms’ to remind individuals about their appointments and to take medications
Majengo Cohort: Success factors • Free condoms, information, promotion and demonstrations on use • Above average comprehensive standard of care offered over the years compared to what's available in MOH clinics • HIV basic care and ARV services provided since 2005 as part of the standard of care • On site ARV/TB and care services • Continuous presence in the area over two decades • Groups success in fund raising
Korogocho Sex Workers Cohort • Established in 1998 • Korogocho;- a poor slum – N/E of the CBD • Targets low socio-economic sex workers • Open cohort with 500 participants enrolled to date • HPV work has been the main research activity but funding has been problematic • Peer led networks and mini baraza’s used to maintain cohort cohesion • Use of cellphone- ‘sms’ reminders on follow-ups and drugs adherence • The ongoing ARV roll out has rekindled follow-up rates in a big way • On site HIV ARV / TB and Care services
Kibera Sex Workers Cohort • Established in 1997 near Kibera slums • Kibera is the ?largest shanty town in Africa • Estimated population 1 million people • We target low socio-economic female sex workers • Mobilized 1500 sex workers with 889 recruited into the trial • Trial - A double blind Azithromycin prophylaxis trial for STI and HIV control • Study conducted between 1998 -2002 • Cohort members not in active follow from 2002 but in touch through peers and cell phone numbers where possible • A dedicated nurse counselor still on site to date for consultations • Peer led networks still used to maintain contacts with most sex workers • Linkages to the ongoing ARV roll out has rekindled interest and follow-up rates high • Cohort members can be re-mobilized within a short time for other studies using the peer leaders
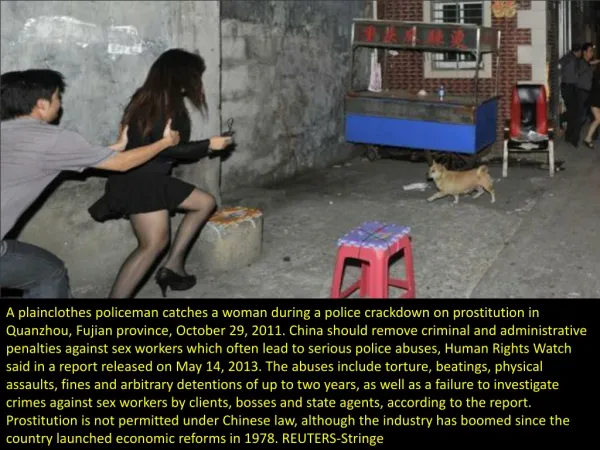
Challenges • Sex work is criminalized in Kenya • No budgetary allocation for STI prevention for vulnerable populations • Number of sex workers in most urban centers unknown • Fluidity in sex work and population highly mobile • ‘Informed consent’ process problematic due to the low level of education • Age of consent is 18 in Kenya yet many sex workers are below that age • Rampant substance abuse (Alcohol) • Drugs for classical STIs not covered by PEPFAR
Challenges • High expectations especially on socio –support among study participants • High maintenance of cohorts • Donor or funding agencies fatigue • Sustainability questions • High cost of air-time for mobile telephony • Coordination at the MOH level lacking – NASCOP and NACC confusion… • No policy or guidelines on way forward beyond PEPFAR supported ARV roll out program by MOH and stakeholders • Fragile public health system (Post election violence) • Weak and inefficient ethics review committee • Experiences not generalizable between clinical trials scenario and cohort studies