Download
1 / 60
600 likes | 606 Views
Osteoarthritis by Dr P.Harischandra on 13/10/2015. Introduction. Osteoarthritis (OA) is the most common type of arthritis. Its high prevalence, elderly , and the high rate of disability related to disease make it a leading cause of disability in the elderly

E N D
Introduction • Osteoarthritis (OA) is the most common type of arthritis. Its high prevalence, elderly, and the high rate of disability related to disease make it a leading cause of disability in the elderly • Aging of populations and because obesity, a major risk factor, is increasing in prevalence.
Osteoarthritis • Osteoarthritis is a non-inflammatory, degenerative condition of joints Characterized by degeneration of articular cartilage and formation of new bone i.e. osteophytes.
Common in weight-bearing joints such as hip and knee. • Commonly affected joints include the cervical and lumbosacral spine, hip, knee, and first metatarsal phalangeal joint (MTP) • But more common in older women i.e. above 50 yrs,particularly in postmenopausal age.
Risk Fators • Obesity esp OA knee • Abnormal mechanical loading eg.meniscectomy, instability • Inherited type II collagen defects in premature polyarticular OA • Inheritance in nodal OA • Occupation eg farmers • Infection:Non-gonococcal septic arthritis • Hereditary • Poor posture • Injured joints • Ageing process in joint cartilage • Defective lubricating mechanism • Incompletely treated congenital dislocation of hip
Primary OA • More common than secondary OA • Cause –Unknown • Common-in elders where there is no previous pathology. • Its mainly due to wear and tear changes occuring in old ages mainly in weight bearing joints.
Secondary OA • Due to a predisposing cause such as: 1.Injury to the joint 2.Previous infection 3.RA 4.CDH 5.Deformity 6.Obesity 7.hyperthyriodism
Crystal Associated OA • Calcium pyrophosphate • dihydrate occurs • mainly in elderly • women, and principally • affects the knee
OA of Premature Onset • Previous meniscectomy • Haemochromatosis
Pathology • OA is a degenerative condition primarily affecting the articular cartilage. 1.articular cartilage 2.Bone 3.Synovial membrane 4.capsule 5.Ligament 6.muscle
ETIOPATHOGENESIS OF OA • Age,gender Local • Genetic OA biochemical effects • Other factors
ETIOPATHOGENESIS OF OA • Dysfunction of joint cartilage • Condrocyte function:1- Degredative enzymes (metalloproteases) 2- Inhibitors Degeneration and regeneration functions are balanced • IL-1 , degredative enzymes + synovial inflammation results:Breakdown of cartilage
PATHOGENESIS OF OA • Cytokines IL-1, IL-6, TNF- • Cell destruction • Membrane phospholipids • Arachidonic acid • Cox-1, Cox-2
IL-1 and metalloproteases have been found to play an important role in cartilage destruction. • Local growth factors,especially transforming growth factor (TGF) are involved in the formation of osteophytes
Articular Cartilage • Cartilage is the 1st structure to be affected. • Erosion occurs,often central & frequently in wt. bearing areas. • Fibrillation,which causes softening,splitting and fragmentation of the cartilage,occur in both wt. bearing & non-wt. bearing areas. • Collagen fibres split and there is disorganisation of the proteoglycon collagen relationship such as H2O is attracted into cartilage, which causes futher softening and flaking.these flakes of cartilage break off and may be impacted b/w the jt.surfaces causing locking and inflammation.
Synovial Membrane • Synovial membrane undergo hypertrophy and become oedematous (which can lead to ‘cold’ effusions). • Reduction of synovial fluid secretion results in loss of nutrition and lubricating action of articular cartilage. Capsule It undergoes fibrous degeneration and there are low-grade chronic inflammatory changes
Undergoes fibrous degernation There is low grade chronic inflammatory changes and acc.to the aspect joint become contracted or elongated. Muscles Undergoes atrophy,as pt. is not able to use the jt. Because of pain which further limits movts. and function. Ligament
Clinical features of OA • Pain • Stiffness • Muscle spasm • Restricted movement • Deformity • Muscle weakness or wasting • Joint enlargement and instability • Crepitus • Joint Effusion
Clinical features 1 • Pain and tenderness • Usually slow onset of discomfort, with gradual and intermittent increase • Pain is more on wt. bearing due to stress on the synovial membrane & later on due to bone surface,which r rich in nerve endings coming in contact. -initially relieved by rest but later on disturb sleep. -Diffuse/ sharp and stabbing local pain
Clinical features • Pain and tenderness (cont) • Types of pain • Mechanical: increases with use of the joint • Inflammatory phases • Rest pain later on in 50% • Night pain in 30% later on
Clinical features 2 • Movement abnormalities • ‘Gelling’: stiffness after periods of inactivity, passes over within minutes (approx 15min.) of using joint again • Coarse crepitus: palpate/hear (due to flaked cartilage & eburnated bone ends) • Reduced ROM: capsular thickening and bony changes in joint,ms. Spasm or soft tissue contracture.
Clinical features 3 • Deformities • Soft tissue swelling: • mild synovitis • small effusions • Osteophytes • Joint laxity • Asymmetrical joint destruction leading to angulation
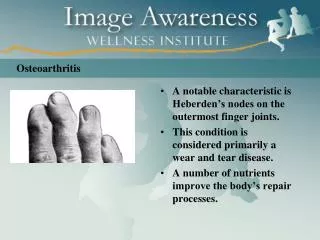
Osteoarthritis of the DIP joints. This patient has the typical clinical findings of advanced OA of the DIP joints, including large firm swellings (Heberden’s nodes), some of which are tender and red due to associated inflammation of the periarticular tissues as well as the joint.
A patient with typical OA of the knees. In the normal standing posture there is a mild varus angulation of the knee joints due to symmetrical OA of the medial tibiofemoral compartments.
Pseudolaxity due to cartilage loss. The joint is not loaded in the first photograph
Unstable distal interphalangeal joints in OA. The examiner is able to push the joint from side to side due to gross instability, a common finding in late interphalangeal joint OA.
Distribution of OA of the hip joint. OA can maximally affect the superior pole, inferior pole, posterior part or other segments of the hip joint. Superior pole involvement, with a tendency for the head of the femur to sublux superolaterally, is the commonest pattern. Involvement of the whole joint (concentric OA) is relatively uncommon.
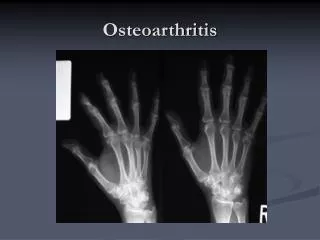
Special Investigations • Blood tests: Normal • Radiological features: • Cartilage loss • Subchondral sclerosis • Cysts • Osteophytes
AIMS OF OA TREATMENT • Pain relief • Preservation and restoration of joint function • Education
Treatment Principles • Education • Physiotherapy • Exercise program • Pain relief modalities • Aids and appliances • Medical Treatment • Surgical Treatment
Education • Nonsystemic nature of disease • Prevent overloading of joint. Obesity!! • Appropriate use of treatment modalities • Importance of exercise program • Aids, apliances, braces • Medial treatments • Surgical treatments
Exercise • Will not ‘wear the joint out’ • Important for cartilage nutrition • Some evidence that lack of exercise leads to progression of OA
Exercise • Encourage full range low impact movements eg swimming, cycling • Avoid • Prolonged loading • Activities that cause pain • Contact sports • High impact sports eg running
Quadriceps exercises for knee OA. Quadriceps exercises are of proven value for pain relief and improving function, and everyone with knee OA should be taught the correct techniques and encouraged to make these exercises a lifetime habit. There is a weight on the ankle.
Use of transcutaneous nerve stimulation (TENS) as an adjunct to other therapy for pain relief at the knee joint. The use of acupuncture, TENS and other local techniques to aid pain relief in difficult cases of OA is often worthwhile.
Aids and appliances • Braces / splints • Special shoes/insoles • Mobility aids • Aids: dressing, reaching, tap openers, kitchen aids • Taping of patella in patello femoral OA