Download
1 / 22
230 likes | 468 Views
Newer cancer therapies Angiotherapy use of agents that inhibit angiogenesis. Angiogenic therapy. Rationale 1) tumour growth is angiogenesis-dependent 2) targets the genetically-stable microvascular endothelial cell 3) anti-angiogenic compounds are cytostatic.

E N D
Newer cancer therapiesAngiotherapyuse of agents that inhibit angiogenesis
Angiogenic therapy Rationale 1) tumour growth is angiogenesis-dependent2) targets the genetically-stable microvascular endothelial cell 3) anti-angiogenic compounds arecytostatic
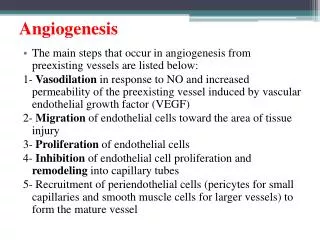
Composition of nascent and mature blood vessel walls • Nascent vessels consist of a tube of ECs, which mature into specialized capillaries, arteries and veins. • (b) Capillaries consist of ECs surrounded by basement membrane and a sparse layer of pericytes embedded within the EC basement membrane. Capillary endothelial layer can be continuous (muscle), fenestrated (kidney/ endocrine glands) or discontinuous (liver sinusoids). The endothelia of the blood-brain barrier or blood-retina barrier are further specialized to include tight junctions, and are thus impermeable to various molecules. • (c) Arterioles and venules have an increased coverage of mural cells compared with capillaries.
Steps in network formation and maturation during embryonic (physiological) angiogenesis
Key differences in tumour vasculature Different flow characteristics / blood volume Microvasculature permeability Increased fractional volume of extravascular, extracellular space
Steps in network formation and maturation during tumour angiogenesis
Cellular mechanisms of tumour angiogenesis 3 (1) host vascular network expands by budding of endothelial sprouts or formation of bridges (angiogenesis); (2) tumour vessels remodel and expand by the insertion of interstitial tissue columns into the lumen of pre-existing vessels (intussusception); and (3) endothelial cell precursors (angioblasts) home from the bone marrow or peripheral blood into tumours and contribute to the endothelial lining of tumour vessels (vasculogenesis) (4) Lymphatic vessels around tumours drain the interstitial fluid and provide a gateway for metastasizing tumour cells. 2 1 4
Angiogenesis-overview Nature Reviews Drug Discovery1, 415-426 (2002)
Angiogenesis-overview • Balance between inhibitory factors (endostatin) and angiogenic factors (VEGF, bFGF) • Tumour cells release pro-angiogenic factors which activate receptors (VEGFR) • also stimulates secretion and activation of MMPs which degrade the basement membrane • This allows activated endothelial cells to migrate towards tumour, helped by integrins • ECs deposit a new basement membrane and secrete growth factors such as platelet-derived growth factor (PDGF), which attract supporting cells to stabilize the new vessel. VEGF – Vascular Endothelial Growth Factor bFGF - basic Fibroblast Growth Factor MMPs – Matrix MetalloProteinases
Angiostatin 38kDa fragment of plasminogen Endostatin 20kDa fragment of collagen XVIII Endothelial cell specific Complete regression in mice No drug resistance ‘cryptic’ angiogenesis inhibitors Inactive until they are released from the parent protein by enzymatic cleavage
Endostatin • Discovered in 1995 by Judah Folkman et al • Phase I clinical trial in 1999 Dr. James Watson predicted that Dr. Folkman would cure all cancer within 2 years Dr. Folkman’s response “If you are a mouse and have cancer we can take good care of you. I respectfully disagree because in our experiments we mostly sacrifice the mice. So, I don't know if that qualifies as taking good care” www.pbs.org/wgbh/ nova/cancer/program.html
Integrins – the ‘velcro’ of the cell • The cell moves by "ruffling" it's membrane. This is done by a series of actin fibers, whose function is controlled by the integrins. These fibers cause the cell membrane to move in certain directions, and the integrins attach to the matrix as this happens, pulling the cell along a micrometer at a time
Representation of the clinical drug development process suggested differences in end points between studies that are targeted at cytotoxic agents compared with studies to test angiogenic modulators DLT, dose-limiting toxicity; MTD, maximum-tolerated dose.
What is in the pipeline? Anti-angiogenic molecules fall into 5 categories • inhibitors of pro-angiogenic growth factors, e.g. VEGF, bFGF, PDGF • protease inhibitors that prevent the breakdown of the surrounding matrix, which is needed for blood-vessel growth; • Analogs of endogenous inhibitors of angiogenesis e.g. endostatin; • inhibitors of cellular adhesion molecules; and • molecules with undefined mechanisms
Anti-VEGFR2 therapy (c,d) Anti-VEGFR2 prunes immature vessels, leading to a progressively 'normalized' vasculature (e) Further treatment leads to a vasculature that is inadequate to sustain tumour growth by day 5. (f) Perivascular cells expressing GFP (under the control of the VEGF promoter) envelope some vessels in the tumour interior. (g) A perivascular cell, presumably a fibroblast, leading the endothelial sprout (arrow).
Imaging studies to monitor tumour angiogenesis (blood flow) Before treatment after treatment Blood-flow maps a | before treatment and b | six months after treatment of a patient with metastatic renal-cell carcinoma with thalidomide.
Haematological malignancies! These images are confocal microscopic sections of bone-marrow biopsies that have been stained with antibody to von Willebrand factor, which highlights blood vessels. In the left panel, normal bone marrow (from a child with a non-neoplastic disease) shows normal microvasculature of uniform-sized vessels. In the right panel, bone marrow from a child with newly diagnosed acute lymphoblastic leukaemia reveals intense neovascularization, with microvessels of variable diameters.
matrix metalloproteinase inhibitors MMPIs • Phase III clinical trials with MMPIs (Marimastat – British Biotech) in several solid tumours • Disappointing results. Reasons may be • Early initiation of advanced testing (Phase III) without the appropriate safety and efficacy indications from Phase I/II trials. • side-effects (mainly musculoskeletal pain) associated with patient non-compliance in trials. • inappropriate model (advanced-stage refractory diseases) in spite of preclinical testing in animal models that had indicated an advantage at an early stage of disease. • Poor survival rate in phase III clinical trials against renal cell carcinoma
References 1) Angiogenesis modulation in cancer research:Novel clinical approaches by M Cristofanilli, C Charnsangavej‡ and GN.Hortobagyi Nature reviews drug discovery VOL 1 JUNE pp 415 (2002) 2) Angiogenesis in cancer and other diseases by P Carmeliet & RK. Jain Nature vol 407 14 september 2000 pp 249 3) Chapter 17 : Knowles and Selby