Download
1 / 35
400 likes | 687 Views
Chapter 38. Medical Nutrition Therapy for Pulmonary Disease. Anatomy of the Pulmonary System. Normal Lung Anatomy. Selected Airway Disorders. Key Terms. Pulmonary aspiration Asthma Bronchopulmonary dysplasia (BPD) Chronic obstructive pulmonary disease (COPD) Cystic fibrosis (CF).

E N D
Chapter 38 Medical Nutrition Therapy for Pulmonary Disease
Key Terms • Pulmonary aspiration • Asthma • Bronchopulmonary dysplasia (BPD) • Chronic obstructive pulmonary disease (COPD) • Cystic fibrosis (CF)
Selected Pulmonary Conditions Having Nutritional Implications
Impact of Malnutrition • Decreased —Vital capacity (lung volume) —Minute ventilation (volume exhaled/minute) —Efficiency of ventilation • Structure and function —Increased compliance (dispensability) —Decreased elasticity —Decreased surfactant
Impact of Malnutrition—cont’d • Pulmonary edema —Decreased O2 transport —Decreased respiratory muscle strength —Decreased energy substrates in the cell —Decreased ventilatory drive with hypoxia —Decreased immune function
Bronchopulmonary Dysplasia Definition: chronic lung disorder seen in early infancy and usually follows intensive therapy for respiratory difficulties in the neonatal period • Assessment —Linear growth —Dietary intake —Gastroesophageal reflux —Chronic hypoxia —Emotional deprivation
Goals of Nutritional Care • Adequate nutrient intakes • Promote linear growth • Maintain fluid balance • Develop age-appropriate feeding skills
Cystic Fibrosis • Inherited autosomal recessive • Epithelial cells and exocrine glands secrete abnormal mucus (thick) • Affects respiratory tract, sweat, salivary, intestine, pancreas, liver, reproductive tract
Diagnosis of Cystic Fibrosis • Neonatal screening provides opportunity to prevent malnutrition in CF infants • Sweat test (Na and Cl >60 mEq/L) • Chronic lung disease • Failure to thrive • Malabsorption • Family history
Nutritional Assessment • List of important assessment points —Significant findings • Recent weight loss or <90% IBW • Is weight fluid or adipose or LBM? • Indirect calorimetry • Edema lowers TP and albumin
Nutritional Assessment in Cystic Fibrosis (From Ramsey BW, et al. Nutritional assessment and management in cyctic fibrosis. A concensus report. Am J Clin Nutr 55: 108, 1992, p.109) * Usually consists of a 24-hour recall with assessment of dietary pattern; should be obtained by a dietician. † Includes both a diet record to determine energy and fat intake as well as a determination of stool fat excretion. this permits calculation of the coefficient of fat absorption (CFA) and assessment of the degree of malabsorption in malnourished patients. ‡ If there is any evidence of iron deficiency, iron status must be measured (I.e., serum iron, iron-binding capacity, and serum ferritin levels).
Nutritional Problems in Cystic Fibrosis • Pancreatic enzyme insufficiency • Malabsorption —Decreased HCO3 secretion —Decreased bile acid reabsorption (fat malabsorption) —Excessive mucus
Symptoms of Cystic Fibrosis Malabsorption • Bulky, foul-smelling stools • Cramping • Obstruction • Rectal prolapse • Liver damage • Other problems —Impaired glucose tolerance
Nutritional Care Goals • Control malabsorption • Provide adequate nutrients for growth Common Treatments • Pancreatic enzyme replacement • Adjust macronutrients for symptoms • Nutrients for growth • Meconium ileus equivalent: intestinal obstruction (enzymes, fiber, fluids, exercise, stool softeners)
Nutrient Needs • Vitamins —H2O soluble need not be increased (exception may be B12) —Fat-soluble – may need a supplement —Sodium: infants need 1/8 to 1/4 tsp/day added salt
Medical Nutrition Therapy • Increase energy intake —Serving size —Snacks —High-calorie foods —Supplements —Night gastrostomy tube feeding with enzymes —TPN only when GI not usable, or in advanced CF (monitor risks of sepsis)
Lung Transplantation • Prior to transplant, children with CF are typically at the 5th percentile for weight
Chronic Obstructive Pulmonary Disease (COPD) • Obstruction of airways —Bronchospasm: asthma —Overproduction of mucus: bronchitis —Destruction of elastin: emphysema —Obstruction: bronchiectasis —Right heart failure: cor pulmonale
Components of Nutritional Assessment for Adults with Chronic Obstructive Pulmonary Disease
Nutritional Status • Nutritional requirements increased from maldigestion, malabsorption • Complications—SOB; coughing; GI distress; anorexia during infections; altered smell; retarded growth
Nutritional Requirements • Energy —HB x AC x IF —1.0-1.2 maintenance —1.4-1.6 repletion • Macronutrient mix —DO NOT OVERFEED! —RQ = CO2/O2 CHO = 1, fat = 0.7, mixed diet = 0.87
Nutritional Requirements—cont’d • Omega-3 fatty acids —May protect smokers from COPD —May be antiinflammatory • Vitamin C supplement for smokers —16-30 mg/d
Treatments • Bronchodilators—theophylline and aminophylline • Antibiotics—secondary infections • Respiratory therapy • Exercise to strengthen muscles
Categories of Medical Nutrition Therapy Management • Routine care • Anticipatory guidance: 90% IBW • Supportive intervention: 85% to 90% IBW • Resuscitative/palliative: below 75% IBW • Rehabilitative care: consistently below 85% IBW • JADA—1997
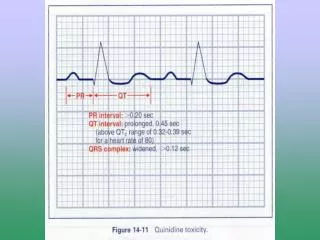
Medical Nutrition Therapy • Monitor side effects of food-drug interactions • Aminoglycosides lower serum Mg++—may need to replace • Prednisone—monitor nitrogen, Ca++, serum glucose, etc.
Cellular Damage • Cellular damage causes oxidative stress. • Excessive accumulation of oxygen free radicals (superoxide anions; hydrogen peroxide; hydroxy radicals; singlet molecular oxygen) • Cellular injury may lead to systemic inflammatory response (SIRS) • Results of trials with antioxidants are mixed.
Oxidative Stress and Critical Illness • Mounting evidence exists that oxidative stress plays a pivotal role in critical illness. • Decreased antioxidant defenses
Respiratory Failure • There may be some benefit to offering antioxidant therapy to patients with respiratory failure. • Studies are ongoing
Respiratory Failure—cont’d • Patient usually on ventilator • Laboratory values indicating RF—ABGs —PCO2 >50 mm Hg (35-45 mm Hg) —PO2 <60 mm HG (80-100 mm Hg) —pH <7.30 (7.35-7.45) —HCO3– (22-26 mEq/L) —O2 saturation >95%
Respirator Weaning • Information monitored —Concentration of inspired O2 (FIO2) —Positive end-expiratory pressure (PEEP) • Nutrition balance important to success —Muscle strength —Albumin levels —RQ —Phosphate depletion corrected
Summary • Pulmonary—affect of nutrition on lungs, and lung status on nutrition • High metabolic rate can occur—will need extra kcal; less from carbohydrate than usual