Download
1 / 45
460 likes | 475 Views
Assessment and Treatment of Benign Intradural Extramedullary Tumors Section: X Chapter: 294 Youmans&Winn Neurological surgery2017 By : Dr. Hamid Nikzad. Benign I ntradural E xtramedullary ( IDEM) tumors; grow beyond the confines of the dura inspite of their name.

E N D
Assessment and Treatment of Benign IntraduralExtramedullary TumorsSection: X Chapter: 294Youmans&WinnNeurological surgery2017By:Dr. HamidNikzad
Benign IntraduralExtramedullary(IDEM)tumors; grow beyond the confines of the durainspite of their name. • In 1887, Sir Victor Horsley performed the first successful resection of a spinal IDEM tumor by laminectomy. • the most part, histologically benign • surgery, is the modality of choice in the management of these tumors
HISTOLOGY AND GROSS PATHOLOGY • The most common tumors : • Meningiomas • Nerve sheath tumors (NSTs; schwannomas and neurofibroma) • Filumterminalemyxopapillaryependymomas
Meningiomas typically arise from the dura mater surrounding the spinal cord and nerves • Histology similar to those seen intracranially • In the spine; the most common histologic subtype is psammomatous variant • prominent and numerous psammoma bodies
Meningiomas have a predilection for the thoracic spine • NSTs can arise from the dorsal or ventral nerve rootlets, dorsal nerve root origin ismore common • Neoplastic Schwann cells stain for the proteins; S-100, vimentin, and Leu-7 • Neurofibromas occur often in patients with neurofibromatosis 1 (NF1) .but can result from sporadic mutations
These lesions stain for S-100 and Leu-7less frequently than do schwannomas • Spinal schwannomas or neurofibromas can be exclusively intradural or exclusively extradural • can involve both compartments as intradural-extradural, or “dumbbell,” tumors • Both schwannomas and neurofibromas are more likely extradural in the cephalad spine and more likely intradural in the caudal spine
Myxopapillaryependymomas are generally confined to the lumbosacral area • Lobulated masses usually found adherent to the filumterminale • These lesions usually diffusely express glialfibrillary acidic protein and vimentin • Paragangliomas are red fleshy tumors that demonstrate synaptophysin on IHC • Neurochemical assessment will show high levels of serotonin
EPIDEMIOLOGY • The most common intradural spinal tumors (both intra- and extramedullary) are meningiomas • Followed by intramedullaryependymoma or NST • Spinal meningiomas account for 12% of all meningiomas • Peak incidence in the sixth to eighth decade of life • Higher incidence in women, ranging from 3:1 to 4.2:1
Younger patients with spinal meningiomas typically havea predisposing factor such as neurofibromatosis2 or prior radiation exposure • Of the two benign NSTs, schwannomas are far more common • NSTs display an equal prevalence in men and women • peak incidence in the fourth and fifth decade of life
Schwannomas most often occur sporadically • Can also occur in conjunction with a syndrome such as NF2, schwannomatosis, or Carney’scomplex • 40% of spinal ependymomas occur in filumterminale • The majority of these are myxopapillary • Occurring with a slight male predilection (1.7 : 1) • Mean age at diagnosis of 36.4 years
Syndromes • IDEM tumors are often seen in conjunction with genetic syndromes such as neurofibromatosis • NF1 is an autosomal dominant syndrome characterized by a mutation in NF1 , the gene coding for neurofibromin on chromosome 17 • often resulting in multiple spinal neurofibromas
NF 2;also displays autosomal dominant inheritance • characterized by a mutation in NF2, the gene coding for merlin on chromosome 22 • can lead to multiple spinal schwannomas, neurofibromas, and spinal meningiomas • NF1 is far more common (1 in 2500 to 1 in 3000) than NF2 (1 in 50,000)
Syndromes predisposing to spinal schwannomas Include: • Schwannomatosis: A syndrome characterized by multiple schwannomas without the defining features of NF1 or NF2 • Carney’s complex: A syndrome characterized by facial pigmentation, cardiac myxomas, endocrine problems, and melanotic schwannomas, 10% of which may be malignant
IMAGING • MRI is the modality of choice to evaluate IDEM tumors. • Usually these lesions display avid contrast enhancement, and meningiomas typically feature a duraltail • CT scan may complement MRI and is well suited for delineating bony anatomy, planning instrumentation, and demonstrating tumor calcification • CT myelography is usually reserved for patients in whom MRI is not possible
Allowing identification of the level of blockage of cerebrospinal fluid (CSF) flow • Plain radiography may display enlarged neural foramina, increased interpediculate distance, vertebral body scalloping , and thinning of the pedicles • Vascular imaging methods ;Angiography, MR Angiography , CT Angiography. may be useful for certain cervical lesions • They allow clear delineation of the relationship of pathology to the vertebral artery
PRESENTATION AND INDICATIONS FOR SURGERY • These benign, slow-growing tumors generally present with pain • Radiculopathy or axial back pain or focal neurological deficits • Compressed nerve roots, myelopathy from spinal cord compression, or caudaequina dysfunction from chronic compression • Spinal instability is less common
Multiple tumors or tumors at young age can present with spinal deformity. • Suspicion of an underlying syndrome, further work-up should include imaging of the entire neuraxis • Symptomatic patients , rapid growth pattern , new neurological deficit should undergo surgery
Surgery in Syndromic Patients • Rapidly growing and symptomatic lesions receive surgery • Much higher intervention for asymptomatic or minimally symptomatic • IDEM tumors encountered in syndromic patients are usually neurofibromas • Makes the potential sacrifice of the involved nerve root • Higher recurrence is in neurofibromatosis patients than sporadic NSTs (39% versus 11%)
SURGICAL CONSIDERATIONS • Mainly, IDEM tumors can be approached via a straightforward posterior, midline incision and laminectomy • surgical challenging: tumors with large extradural components (dumbbell ,purely extradural) tumors whose excision requires extensive bone removal that may require instrumentation multicompartmental tumors (dumbbell), anteriorly or ventrally tumors malignant or adherent/invasive tumors Tumors involved functional nerve root
Electrophysiology • Electrophysiology is commonly employed for any lesion with an intradural component • Standard monitoring techniques including : Somatosensory evoked potentials Motor evoked potentials of the upper and lower extremities • The decision to sacrifice cervical or lumbosacral nerve roots remains a challenge • Considerations are less important in the thoracic spine
Approaches • The vast majority of IDEM tumors can be addressed through a standard posterior midline approach andlaminectomy • Particularly favored for intradural pathology • Given the relative ease of dural repair • Anterior and lateral approaches are used to large extravertebral components of dumbbell tumors
Cervical Approaches • Most approach to lesions located anterolaterally, laterally, or posterolaterally is midline approach with laminectomy or laminaplasty • The posterior approach avoids encounter with major vessels or visceral structures • For subaxial cervical lesions located ventral to the spinal cord, anterior approaches have been described • For low cervical lesions, cervicothoracic junction lesions, a modified anterior or trap-door exposure, a anterior approach, partial median sternotomy, and anterolateralthoracotomy, to allow bilateral or unilateral exposure of the spine as low as the third thoracic vertebra
Thoracolumbar Approaches • For thoracic IDEM tumors not suited to a posterior midline approach, lateral approaches are favored • Anterior approaches in the thorax are limited by vital vascular structures and the mediastinum • Extracavitary approach : • For traumatic injuries to the anterior thoracic spine • For ventrally situated thoracic IDEM tumors with large extraforaminal extension.
Lumbosacral Approaches • Posterior approaches: For lower lumbar ,primarily intradural lesions • retraction injuy to the spinal cord is less of a concern • Retroperitoneal approaches: for lower lumbar spine are problematic because they traverse the psoas muscle place the lumbosacral plexus at risk limited by the presence of the iliac crest involvement of a general surgeon may be required
For intradural pathology in sacral region: Posterior midline sacral approaches • For extradural pathology sacral region: anterior and posterior approaches with the involvement of a colorectal surgeon • Generally, bladder and bowel function is preserved if S2-S4 are intact on at least one side.
Need for Spinal Fusion • In posterior midline approach, resection of lesions with extradural components often necessitates extendedlaminectomies and graded or completefacetectomies on the side • Aggressive bone removal, although necessary to achieve oncologic benefit, may introduce mechanical instability and supplemental instrumented fusion and arthrodesis are necessary • Medial facetectomies even bilaterally performed do not introduce significant spinal instability, unilateral complete facetectomies can introduce significant instability in the lumbar or cervical
SURGERY FOR INTRADURAL NERVESHEATH TUMORS • Patients undergoing surgery for NSTs should receive intravenous steroids preoperatively • For NSTs with intradural components, somatosensory evoked potentials and motor evoked potentials should be monitored • For NSTs involving the C5-T1 and L2-S4 nerve roots, continuous EMG and evoked EMG monitoring should be considered
For standard, posterior midline approaches, patients are placed in the prone position • For lesions aboveT1, a Mayfield head holder may be employed for adequate stabilization of the cervical spine • For lesions aboveT6, the patient should be placed on chest bolsters with the shoulders tucked • Lesions belowT6 will require the shoulder to be abducted 90 degrees and may require an open-frame spine table for adequate visualization
For intradural lesions that do not cross the midline, a hemilaminectomy can be entertained • but full laminectomy or laminaplasty should be performed for posteriorly situated lesions crossing the midline • Lateral or ventrolateral lesions will likely require facetectomy,which should be supplemented with instrumentation and fusion
NSTs most often arise from dorsal nerve roots • This pattern is not always observed, and even when it is, the anatomy can be distorted and unclear • EvokedEMG is particularly useful for identifying efferent motor roots • Afferent nerve roots are often enlarged, longested, and hypervascular, whereas efferent nerve roots can appear entirely normal
Preservation of uninvolved ventral nerve roots is particularly important in cervical and lumbosacral regions • dorsal roots can usually be sacrificed without deficit • In the upper cervical spine, the surgeon should be ware of spinal accessory nerve rootlets coursing superior and anterior to the denticulate ligament in a cephalad course
For schwannomas, it is usually possible to separate individual fascicles from the tumor, and smaller tumors may be excised in one piece • whereas larger tumors may require debulking • Neurofibromas usually lack a plane and are inseparable from their nerve root of origin. • in the cervical and lumbar spine, debulking with preservation of anterior rootlets may be best if the nerve root is found to be functional, • whereas roots that are confirmed to be nonfunctional with • intraoperative stimulation can be sacrificed
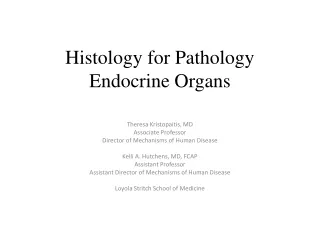
T9 T10 B A Thoracic schwannoma. A, T1-weighted, contrast enhanced sagittal magnetic resonance image (MRI) demonstrates a large intradural mass at T9-T10. B, Axial MRI demonstrates the large size of this lesion, causing a high degree of spinal cord compression. This patient had gait ataxia and left-sided thoracic pain.
SURGERY FOR DUMBBELL TUMORS AND EXTRADURAL NERVE SHEATH TUMORS • NSTs have a significant extradural component, (purely extradural or intradural-extradural dumbbell tumors), the origin is intradural segment of a dorsal or ventral nerve root • Intradural exposure first, because resection of the intradural component will decompress the spinal cord and release the neural elements from adhesions to the tumor capsule • Avoiding traction injury during manipulation of the extradural tumor component
When the C1 root is involved, a small craniotomy may be needed • In the thoracic spine, additional removal of the transverse process and rib head may be required as part of a lateral extracavitary approach for the extraforaminal component • In the lumbar spine, opening of the intertransverse membrane may be required for removing a paraspinal tumor • During extradural tumor resection, it is important to stay on the tumor capsule to avoid epidural and foraminal bleeding as well as the perivertebral venous plexuses
SURGERY FOR SPINAL MENINGIOMAS • Anteriorly located tumors are common • Debulking and a gross total resection are feasible from a posterior laminectomy • Meningiomas have an enplaque involvement of the dura, and the exact amount of dura that needs to be resected for a complete free margin is difficult to determine • Ventrally tumors, anterior approaches can be performed in the cervicalspine and are unnecessary in the lumbar spine
intradural nerve roots can be retracted without concern • Anterior approaches are particularly complicated in the thoracic region • upper thoracic lesions may be accessed through a trap-door approach or parascapularextrapleural approach • For the remainder of thoracic lesion, extracavitary or retropleural approaches are employed, if a traditional posterior midline approach is not suitable.
SURGERY FOR TUMORS OF THE FILUM TERMINALE • Filumterminale tumors (myxopapillaryependymoma and paraganglioma), en bloc resection is often preferred • Great care is taken to avoid piecemeal debulking of the lesion • This has been associated with increased rates of local failure and upward seeding or CSF metastasis • The most common lesion encountered is myxopapillaryependymoma,with paragangliomas being far more rare
Myxopapillaryependymomas tend to be solidfleshy tumors amenable to en bloc resection • Paragangliomas very vascular and more adherent to surrounding nerves • Careful microdissection from adjacent caudaequina nerve roots is required to free the tumor of adhesions • Filum is identified and tested with a neurostimulator in similar fashion to a standard tethered cord release
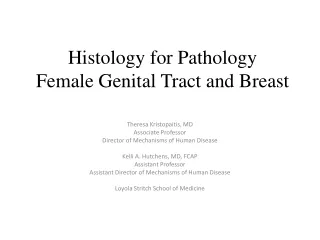
Myxopapillaryependymoma. A, Sagittal T1-weighted magnetic resonance imaging with contrast shows an intramedullaryenhancing mass at T12-L1 and L2. B,Sagittal T2-weighted image demonstrating significant displacement of the caudaequina at the L1-L2 level
ADJUVANT THERAPY AND RADIOSURGERY • Chemotherapy and conventional radiotherapy do not have a significant role in the management of spinal NSTs and meningiomas • For multiply recurrent spinal meningiomas or meningiomas with atypical or malignant histology, radiation doses of 50 to 54Gy in 1.8-to 2-Gyfractions • Spinal radiosurgery has introduced a new potential therapy for IDEM tumors , if proven effective, represents a far less invasive alternative to surgical resection
Spinal myxopapillaryependymoma, adjuvant radiotherapy has a more defined role • Adjuvant radiotherapy following surgery associated with significantly improved regardless of whether resection was total or subtotal • The adjuvant radiotherapy is intensity-modulated radiation therapy with treatment fields including ; thecal sac, sacroiliac joints, and meningeal sleeves within intervertebral foramina
OUTCOMES • When GTR is achieved, surgical outcomes for spinal meningiomas are quite good. • Risk factors for recurrence include: - invasion of the pia - Simpson resection grade - histologic grade • Spinal meningiomas in patients under 50 years of age have been observed to recur at a higher rate and carry a worse prognosis
Increased proportion of younger patients with tumors secondary to syndromes or radiation exposure • Spinal NSTs in the setting of NF1 and NF2, significant risk factors associated with tumor recurrence include: - NF2 - Old age - Subtotal removal - Surgery for a recurrent tumor
Tanks for attention Any question?