Download
1 / 39
390 likes | 742 Views
CASE 1. Medenilla – Miranda C2 Group #1. Case 1. Patient: 12 y/o boy CC: severely pruritic papules on the hands and feet. HPI. 1 month PTC pruritic erythematous papules, some topped by a vesicle over the sides of the fingers and toes

E N D
CASE 1 Medenilla – Miranda C2 Group #1
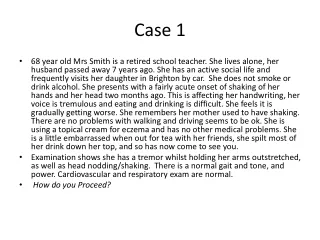
Case 1 • Patient: 12 y/o boy • CC: severely pruritic papules on the hands and feet
HPI 1 month PTC pruritic erythematous papules, some topped by a vesicle over the sides of the fingers and toes lesions gradually spread to axillae and inguinal areas wakes up at night because of severe pruritus younger brother and sister of the patient are beginning to have similar symptoms Consultation
PE • Multiple erythematous to hyperpigmented papules • mostly excoriated • Diameter Size: 0.3 to 0.6 cm • Areas of Predilection: the anterior and posterior trunk both axillae umbilicus inguinal areas elbows wrist fingerwebs toewebs
Salient FeaturesSubjective • Pruritic erythematous papules on the fingers and toes which spread to the axillae and inguinal areas • Pruritus - more prominent at night • Siblings were noted to have similar symptoms
Salient FeaturesObjective • multiple erythematous to hyperpigmented papules • mostly excoriated • Diameter Size: 0.3 to 0.6 cm • Areas of Predilection: anterior and posterior trunk both axillae umbilicus inguinal areas elbows wrist fingerwebs toewebs
Differential Diagnosis • Pediculosis • Milaria Rubra • Insect Bites
Pediculosis • Three varieties of flattened, wingless insects that infest humans • Pediculus humanus var. capitis (head louse) • Pediculus humanus var. corporis (body louse) • Phthirus pubis (pubic or crab louse)
Differential Diagnosis Presentation Patient Pediculosis capitis • Lesion • Intense pruritus – scalp • Excoriations in the scalp • Secondary impetigo • Age of Predilection • Principally – children • May occur in adults • Area of Predilection • scalp • Etiology • Pediculushumanus var. capitis • Lesion • Multiple pruriticerythematous and hyperpigmented papules • Age • 12 years old • Area of Lesion • Sides of fingers and toes • Gradually spread – trunk, axillae and inguinal areas • Umbilicus, elbows, wrists, fingerwebs and toewebs • Others • Wakes up at night because of severe pruritus • Brother, sister having similar symptoms
Differential Diagnosis Presentation Patient Pediculosis capitis • Lesion • Pruritus • Erythematousmacules / urticarial wheals • Excoriated papules • Area of Predilection • Upper back • (-) hands and feet • Hallmark • Hyperpigmented, parallel stretch marks • Etiology • Pediculushumanus var. corporis • Lesion • Multiple pruritic erythematous and hyperpigmented papules • Age • 12 years old • Area of Lesion • Sides of fingers and toes • Gradually spread – trunk, axillae and inguinal areas • Umbilicus, elbows, wrists, fingerwebs and toewebs • Others • Wakes up at night because of severe pruritus • Brother, sister having similar symptoms
Presentation Patient Differential Diagnosis Pediculosis pubis • Lesion • Maculae cerulae – blue or slate-colored macules • Non-pruritic • May include sides of the trunk, inner aspects of thigh • Age of Predilection • adults • Area of Predilection • Genital region • Hypogastrium • Rarely, axillae and eyelashes • Etiology • Pthirius pubis • Lesion • Multiple pruritic erythematous and hyperpigmented papules • Age • 12 years old • Area of Lesion • Sides of fingers and toes • Gradually spread – trunk, axillae and inguinal areas • Umbilicus, elbows, wrists, fingerwebs and toewebs • Others • Wakes up at night because of severe pruritus • Brother, sister having similar symptoms
Mosquito bites Common cause of papular urticaria Sever local reactions are seen in young children with immunodefficiency Hypersensitivity reactions may occur
Ants Sting Pustules, blisters formed following fire ant sting on hand, arm, leg and ankle. Painful,burning sting, whealing Intense pruritic sterile pustules develop at the site
Caterpillar Dermatitis Irritation is produced by the hair (toxins)coming in contact with the skin. Severe pain, local pruritic erythematous macules and wheals May cause widespread persistent dermatitis
Scabies • Caused by the itch mite, Sarcoptes scabiei • Characteristics • Pruritic papular lesions, excoriations & burrows • Eczematization, lichenification, impetigo and furunculosis maybe present • Dull Red nodules may appear during active scabies; these are 3-5 mm and may or may not itch
Scabies • Severe itching begins with the sensitization of the host • Itching is most intense at night • During the day- pruritus is tolerable • Women - itching of nipples associated with generalized pruriticpapular eruption • Men – Itchy papules in the scrotum
Sites of Predilection • Fingerwebs, wrists, axillae, areolae, umbilicus, lower abdomen, genitals, buttocks • Circle of Hebra - Imaginary Circle intersecting the main sites of involvement –axillae, elbows flexure, wrist and hands and crotch • Adults- Scalp and face are usually spared • Infants- commonly present over entire cutaneous surface
Transmission • Overcrowding and close living quarters • Common use of contaminated linen and clothing **when more than one member of the family has pruritus, a suspicion of scabies should be aroused
Diagnostic Test A positive diagnosis is made by the demonstration of the mite under the microscope To identify the burrows quickly, a drop of india ink and giemsa violet can be applied to the infested area, then removed with alcohol --thin threadlike burrows retain the ink
Benzyl benzoate 6-10% precipitated sulfur in white petrolatum - Rubbed into skin from neck to the feet especially to the creases, perianal areas, umbilicus, and free nail edge and folds - Washed off 8-10 hrs later
Permethrin 5% cream - Most widely used - Lethal to mites but has low toxicity for humans • Lindane benzene hexachloride - Rarely used as a 1st line agent
Crotamiton - Lower cure rates but when used, it should be applied on 5 successive nights and washed off 24 hrs after last use
Ivermectin - Available in 3 and 6 mg pills at a dose of 200 mcg/kg - Oral treatment is effective but in crusted type of scabies, it should be used with a topical agent - Repeated 2 or 3 times at intervals of 1-2 wks - Has good margin of safety but neurotoxicity may be possible
Management • Individuals with close contact should also be treated • Avoid close personal contact with affected person • Clothing and bed linen should be changed and laundered thoroughly