Download
1 / 33
450 likes | 974 Views
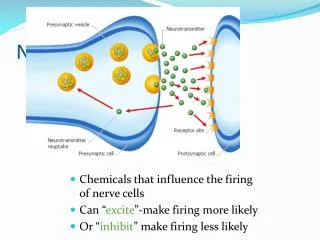
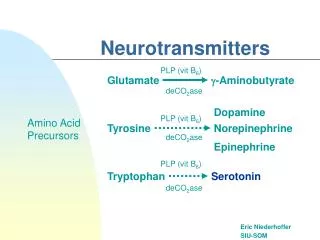
Monoamine neurotransmitters (+ Acetylcholine and Histamine). Paul Glue. Biogenic amines/monoamines. Cortical Innervation - Monoamine Pathways. Common features: Cell bodies arising in upper brainstem Radiate to most cortical areas Intense arborization of dendritic terminals

E N D
Monoamine neurotransmitters(+ Acetylcholine and Histamine) Paul Glue
Cortical Innervation - Monoamine Pathways Common features: Cell bodies arising in upper brainstem Radiate to most cortical areas Intense arborization of dendritic terminals Consistent with modulatory role Common features: Cell bodies arising in upper brainstem Radiate to most cortical areas Intense arborization of dendritic terminals Consistent with modulatory role DOPAMINE NOREPINEPHRINE NE Ventral Tegmental Area Substantia Nigra Substantia Nigra DOPAMINE DOPAMINE • Common features: • Relatively small numbers of cell bodies arising in upper brainstem • Radiate to most cortical areas • Intense arborization of dendritic terminals • Consistent with modulatory role on other cortical synapses SEROTONIN
(A9) (A10) (A10) (A9) Dopamine Pathways in the Brain • Localization: • - nigrostriatal: substantia nigra (A9) striatum • - mesolimbic: ventral tegmental area (A10) limbic structures • - tuberoinfundibular pathway pituitary • Effects/timecourse: • - nigrostriatal: initiation and control of voluntary movement • - mesolimbic: interactive and reactive behavior • - tuberoinfundibular: prolactin, GH secretion
Dopamine receptors • Density in CNS: D1>D2>D3>D4>D5 • D1, D5 linked to adenylate cyclase • D2, D3, D4 (not linked to AC) • Functions: • Only D2 antagonism linked to antipsychotic effects • D2/3 agonists for Parkinson’s Disease • D1 antagonists ?anticraving effects • No known function for D4/5 ligands
Functions of DA in the brain • Motor control: movement initiation and cessation • Reward/Motivation: dependence liability of compounds correlated with degree of DA release in Nucleus Accumbens • Endocrine: Inhibition of prolactin release • Mood: DA releasers/reuptake inhibitors (e.g. cocaine, amphetamine) cause euphoria; D2 antagonists – anhedonia in HVs • Psychosis: DA releasers/reuptake inhibitors may produce psychotic symptoms (paranoid delusions; hallucinations; etc); all antipsychotics are D2 antagonists • Sleep:VTA inhibits ventrolateral preoptic area • Attention/Learning/Working memory
Peripheral DA activity • Blood vessel smooth muscle beds (vasorelaxation) • Atria ( myocardial contractility, cardiac output) • Kidneys (nephrons, prox tubule epithelium) – sodium excretion • Gut wall plexus • Lymphocytes
Parkinson’s Disease and Dopamine • Symptoms: • tremor; rigidity/stiffness; bradykinesia; postural imbalance • Rates • onset in 50’s; highest in elderly; protracted course with high disability/morbidity; dementia 25-40% • Pathophysiology: • loss of nigrostriatal dopaminergic neurons • MPTP (DA neurotoxin) produces PD • Treatment: • Increase synaptic dopamine concentrations • (L-DOPA; DA agonists; MAO-B/COMT inhibs) • gradual loss of efficacy over time • Side effects of treatment: • Dyskinesia; psychosis, nausea 18F-L-DOPA PET image
Schizophrenia and Dopamine • Symptoms:delusions; hallucinations; disturbances of thought; bizarre behavior; personality change; apathy; withdrawal; etc; episodic or progressive patterns • Rates:peak onset in late teens-early 30’s; ~ 1% lifetime prevalence • Pathophysiology: • mesolimbic dopaminergic dysfunction/overactivity (hypothesized) • cocaine/amphetamine produce psychotic symptoms • increased DA release relative to controls (no differences in brain DA concs, DA receptor density, etc.) • Treatment: • All effective drugs are dopamine D2 antagonists (+ other pharmacological effects); potency correlates with daily dose • Side effects: • Tremor, stiffness; restlessness; akathisia Laruelle M, Biol Psych 1999
Relationship between D2 antagonist potency and average daily dose
Dopaminergic Effects/Side Effects • Drugs that increase DA neurotransmission ( synaptic DA) • most are effective symptomatic treatments for PD • may precipitate/worsen psychosis/dyskinesia • potentially addictive • other s/e: nausea, GI symptoms • Postsynaptic agonists (DA from L-DOPA; bromocriptine, pramipexole) • Inhibitors of enzymes which degrade DA (MAOIs (selective MAO-B-I: deprenyl); COMT inhibitors (entocapone) • Inhibitors of DA reuptake or inducers of DA release (cocaine, d-amphetamine - not yet shown to help PD) • Block DA neurotransmission (postsynaptic antagonism) • worsen PD; may induce reversible Parkinsonian sx • improve psychotic symptoms • antiemetic, prokinetic • Typical neuroleptics - D2 antagonists (haloperidol etc plus newer agents) • Atypical neuroleptics (D2 antagonism + ?: clozapine)
Norepinephrine Pathways in the Brain dorsal bundle ventral bundle • diffuse innervation of most cortical and subcortical areas • extensive distribution in blood vessels, lungs, heart, urethra, GI tract • Effects/timecourse: • inhibit/facilitate spontaneous neuronal discharge; • slow onset and long duration; • modulatory • Receptors: • 1, 2 and subtypes; 1, 2, 3
Agonist effects at NE receptors • 1: • 2: • 1: • 2: • 3: • Smooth muscle contraction (blood vessels, urethra, bronchioles, etc) • Central autoreceptor (presynaptic inhibition of NE release) • Endocrine ( insulin, glucagon release in pancreas) • GI (sphincter contraction) • Platelet aggregation • Increased cardiac output (contractility, • Endocrine (ghrelin, renin secretion) • Smooth muscle relaxation (uterus, bladder, blood vessels, bronchi • Lipolysis • Lipolysis NE in the periphery: sympathetic nervous system (fight or flight)
Functions of NE in the brainDisorders associated with altered central NE • Alertness/Arousal/Sleep: • LC inhibits ventrolateral preoptic area • Memory • Mood • Attention/Learning/Working memory • Depression • Anxiety/panic disorder • NE= anxiety; MHPG concs (NE metabolite) correlate with anxiety • ADHD • Schizophrenia • Akathisia (+); negative symptoms (-)
NE Effects/Side Effects • Increase NE neurotransmission by increasing synaptic NE • most are effective symptomatic treatments for major depression • may cause adrenergic side effects (increased blood pressure, heart rate, dry mouth, tremor) • Presynaptic reuptake blockers (imipramine; venlafaxine; etc; cocaine is not!) • Indirect effects on NE neurotransmission (fluoxetine and other SSRIs - neuronal crosstalk; lithium and ECT) • Enzyme inhibitors (MAOIs:phenelzine etc) • Decrease NE neurotransmission • risk of inducing or worsening depression • adrenergic side effects sedation, bradycardia, hypotension (esp. postural), bronchoconstriction • Inhibit NE formation/release (reserpine; a-methyldopa) • Post-synaptic b-adrenoceptor antagonists (e.g. propranolol - uncommon)
5HT Pathways in the Brain • ascending - raphe nuclei (pons/upper brain stem) and • descending - medullary cell bodies • diffuse fibers innervate many cortical/subcortical structures • extensive location in gut (enterochromaffin cells), platelets, etc • Effects/timecourse: • inhibit/facilitate spontaneous neuronal discharge; • slow onset and long duration; • modulatory • Receptors: • 14 identified; 5HT1-7 plus subtypes cord
14 serotonin receptors in 6 families FamilyTypeMechanismPotential 5-HT1 Gi/Go-protein coupled. Decreases cAMP. Inhibitory 5-HT2 Gq/G11-protein coupled. Increases IP3 and DAG. Excitatory 5-HT3 Ligand-gated Na+ and K+ Depolarizing plasma Excitatory cation channel. membrane. 5-HT4 Gs-protein coupled. Increases cAMP. Excitatory 5-HT5 Gi/Go-protein coupled.Decreases cAMP. Inhibitory 5-HT6 Gs-protein coupled. Increases cAMP. Excitatory 5-HT7 Gs-protein coupled. Increases cAMP. Excitatory
Serotonin 1/2 receptors • 5HT1a: buspirone (partial agonist) – anxiolytic, antidepressant • 5HT1b: triptans (agonists) – vasoconstriction; antimigraine (5HT1c – no such receptor) • 5HT1d: triptans (agonists) – vasoconstriction; antimigraine • 5HT1e: methysergide - ? effect • 5HT1f: triptans (agonists) – vasoconstriction; antimigraine • 5HT2a: LSD, psilocybin (agonists) – perception SGAs (antagonists) - ?reduced EPSE • 5HT2b: Fenfluramine (agonist) anorexia Tegaserod (antagonist) - reduced GI motility/IBS • 5HT2c: Mirtazapine (antagonist) - anxiolytic.antidepressant
Serotonin 3-7 receptors • 5HT3: ondansetron (antagonist) – anti-nausea, vomiting • 5HT4: cisapride, tegaserod (agonists) - altered GI motility • 5HT5a: ? function • 5HT6: ? function • 5HT7: ? function
Drugs that modulate 5HT • Increase 5HT neurotransmission by increasing synaptic 5HT • most are effective symptomatic treatments for major depression • may cause serotonergic side effects (nausea/GI discomfort; anxiety; tremor; insomnia) • Selective presynaptic reuptake blockers ( SSRIs fluoxetine; paroxetine; etc) • Nonselective presynaptic reuptake blockers (imipramine etc) • Indirect effects on 5HT neurotransmission (lithium and ECT) • Enzyme inhibitors (MAOIs: phenelzine etc) • Decrease 5HT neurotransmission • Most serotonin antagonists have no obvious side effects • Subtype selective effects may affect GI motility, nausea, vomiting, EPSE • General 5HT depletion risk of inducing or worsening depression • experimental depletion of brain 5HT (L-tryptophan-free amino acid drink)
Monoamine transporters (Example - SERT) A brief history: - 1961: Axelrod: presynaptic uptake of neurotransmitter first reported - 1979: Raisman: SERT is a target for antidepressant drugs - 1981: Langer: linking of SERT to depression - 1991: Blakely: sequence of the transporter gene from rats published
SERT is a member of the neurotransmitter transporter family • Neurotransmitter transporters belonging to the solute carrier 6 (SLC6) family, including: • γ-aminobutyric acid (GAT) • norepinephrine (NET) • serotonin (SERT) • dopamine (DAT) transporters • All are Na+, Cl–-dependent transporters with 12 transmembrane segments • Primary function: following neurotransmission, to reset neuronal signaling by transporting neurotransmitter out of the synapse and back into the pre-synaptic neuron
SERT in action High affinity antidepressant binding site in extracellular pocket ?Low affinity binding site on intracellular domain 5HT K+ Na+ Cl- 5HT Na+ Cl-K+
Monoamine transporters and psychotropics Reuptake Inhibitors: (not substrates for the transporter) SSRIs Mixed monoamine reuptake inhibitors Psychostimulants Substrates: (release 5HT after being taken up by SERT) Amphetamine Fenfluramine Ecstacy/MDMA mCPP (trazodone metabolite)
Histamine • Brain histamine neurons arise in tuberomammillary nucleus in the posterior hypothalamus. • Project throughout the nervous system • May stimulate the cerebral cortex either directly or indirectly (5HT, ACh, galanin, GABA, substance P etc) • 4 receptors (H1-4) • Histamine is arousing/excitatory; increased release in stressed animals; associated with anxiety related behaviours (no human data)
Histaminic drugs • H1 antagonists: antiallergy/ local antiinflammatory effects • H2 antagonists: reduced gastric acid secretion • H3 (antagonists) – may enhance transmission of monoamines, histamine – experimental • H4: ??
Acetylcholine • Localization: • 8 cell groups which project diffusely to all cortical/ subcortical areas • main cortical projection: Nucleus Basalis of Meynert • Effects/timecourse: • slow onset; prolonged regulatory/modulatory effects on other neuronal activity • Receptors: • muscarinic M1-M5 (G-protein coupled) • majority of brain ACh receptors • nicotinic (ligand-gated ion channel; multiple subunit combinations; neuromuscular and ganglionic subtypes)
ACh receptor localization Agonists Learning/memory GI motility, nausea HR (vagal tone) vasodilation; bladder contraction salivation broncho-constriction +/- (dose dependent) +/- (dose dependent) attention, performance; tremor Antagonists memory impairment GI motility, constipation HR urinary hesitancy; blurred vision dry mouth paralysis Brain (m1-5) Autonomic ganglia (m1) Heart (m2) Smooth muscle (m2, m3) Exocrine glands (m3) Lung (m4) Autonomic NS (n) Skeletal muscle (n) Brain (n)
Functions of ACh in the brain • Learning and memory • anticholinergics and ACh lesions impair learning and memory • Attention/arousal • Pain (?) • Schizophrenia (?sensory gating) • (peripherally) • striated muscle activation • autonomic innervation • parasympathetic NS
Cholinergic Side Effects • Muscarinic antagonists [nonselective neuroleptics, antidepressants] • impair memory • symptoms of peripheral cholinergic blockade • constipation • urinary hesitancy • blurred vision • dry mouth • Muscarinic agonists • nausea, diarrhea • drooling • improved attention, memory
Therapeutic ACh Compounds • Cholinesterase inhibitors (donepezil; rivastigmine; galanthamine) • increase brain [ACh]; improves memory, attention in Alzheimer’s dis. • [organophosphorus insecticides (e.g. Malathion) and nerve gas (Sarin)] • Muscarinic antagonists • orphenadrine, procyclidine, others - tremor in Parkinson’s disease • scopolamine - pre-anesthesia • Muscarinic agonists • pilocarpine - glaucoma; • (experimental for Alzheimer’s disease) • Nicotinic agonists (nicotine) • improves memory; addictive (via DA) • Nicotinic neuromuscular blocking agents • tubocurarine; pancuronium, others - surgical paralysis