Download
1 / 1

E N D
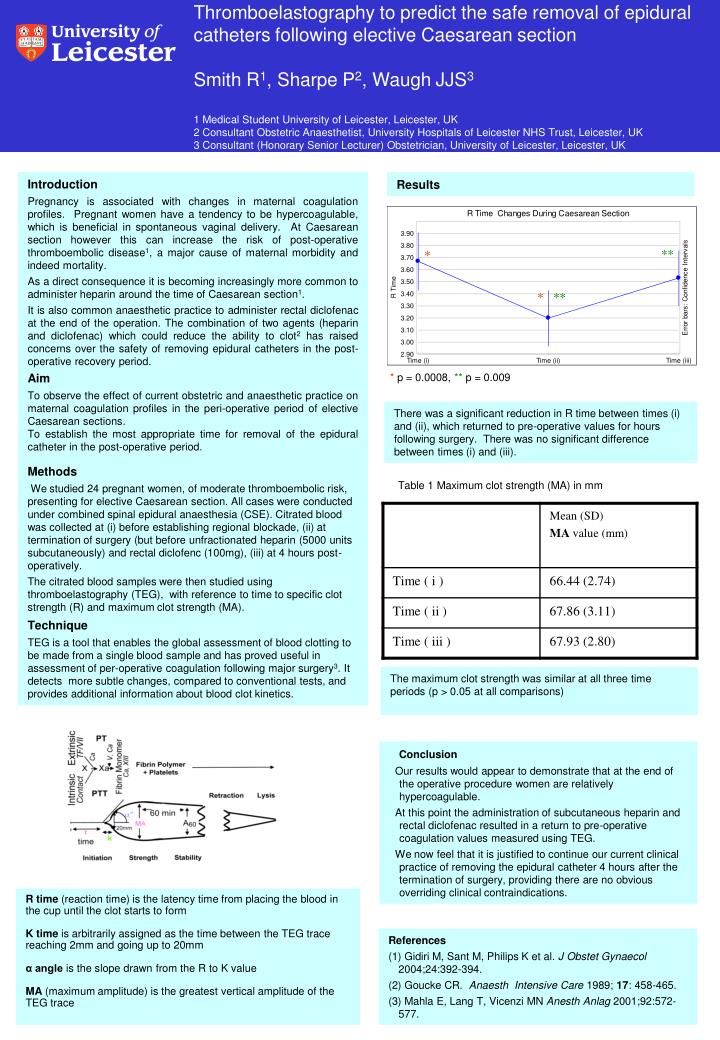
Thromboelastography to predict the safe removal of epidural catheters following elective Caesarean sectionSmith R1, Sharpe P2, Waugh JJS31 Medical Student University of Leicester, Leicester, UK2 Consultant Obstetric Anaesthetist, University Hospitals of Leicester NHS Trust, Leicester, UK3 Consultant (Honorary Senior Lecturer) Obstetrician, University of Leicester, Leicester, UK Introduction Pregnancy is associated with changes in maternal coagulation profiles. Pregnant women have a tendency to be hypercoagulable, which is beneficial in spontaneous vaginal delivery. At Caesarean section however this can increase the risk of post-operative thromboembolic disease1, a major cause of maternal morbidity and indeed mortality. As a direct consequence it is becoming increasingly more common to administer heparin around the time of Caesarean section1. It is also common anaesthetic practice to administer rectal diclofenac at the end of the operation. The combination of two agents (heparin and diclofenac) which could reduce the ability to clot2 has raised concerns over the safety of removing epidural catheters in the post-operative recovery period. Aim To observe the effect of current obstetric and anaesthetic practice on maternal coagulation profiles in the peri-operative period of elective Caesarean sections. To establish the most appropriate time for removal of the epidural catheter in the post-operative period. Methods We studied 24 pregnant women, of moderate thromboembolic risk, presenting for elective Caesarean section. All cases were conducted under combined spinal epidural anaesthesia (CSE). Citrated blood was collected at (i) before establishing regional blockade, (ii) at termination of surgery (but before unfractionated heparin (5000 units subcutaneously) and rectal diclofenc (100mg), (iii) at 4 hours post-operatively. The citrated blood samples were then studied using thromboelastography (TEG), with reference to time to specific clot strength (R) and maximum clot strength (MA). Technique TEG is a tool that enables the global assessment of blood clotting to be made from a single blood sample and has proved useful in assessment of per-operative coagulation following major surgery3. It detects more subtle changes, compared to conventional tests, and provides additional information about blood clot kinetics. Results ** * * ** * p = 0.0008, ** p = 0.009 There was a significant reduction in R time between times (i) and (ii), which returned to pre-operative values for hours following surgery. There was no significant difference between times (i) and (iii). Table 1 Maximum clot strength (MA) in mm The maximum clot strength was similar at all three time periods (p > 0.05 at all comparisons) Conclusion Our results would appear to demonstrate that at the end of the operative procedure women are relatively hypercoagulable. At this point the administration of subcutaneous heparin and rectal diclofenac resulted in a return to pre-operative coagulation values measured using TEG. We now feel that it is justified to continue our current clinical practice of removing the epidural catheter 4 hours after the termination of surgery, providing there are no obvious overriding clinical contraindications. R time (reaction time) is the latency time from placing the blood in the cup until the clot starts to form K time is arbitrarily assigned as the time between the TEG trace reaching 2mm and going up to 20mm α angle is the slope drawn from the R to K value MA (maximum amplitude) is the greatest vertical amplitude of the TEG trace References (1) Gidiri M, Sant M, Philips K et al. J Obstet Gynaecol 2004;24:392-394. (2) Goucke CR. Anaesth Intensive Care 1989; 17: 458-465. (3) Mahla E, Lang T, Vicenzi MN Anesth Anlag 2001;92:572-577.






