Download
1 / 49
570 likes | 1.19k Views
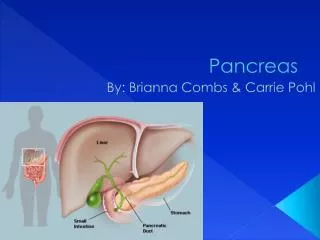
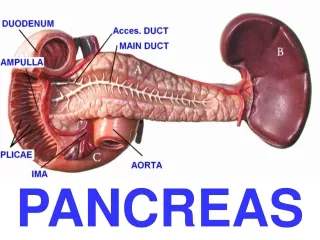
Pancreas Cancer. Richard Zubarik, MD Professor of Medicine Director of Endoscopy. Pancreas Anatomy. Physiology. Ductal cell Bicarbonate, water , digestive enzyme secretion. Islets of Langerhans Hormones secreted directly into blood flow Alpha cell-glucagon Beta cell- insulin and amylin

E N D
Pancreas Cancer Richard Zubarik, MD Professor of Medicine Director of Endoscopy
Physiology Ductal cell Bicarbonate, water , digestive enzyme secretion Islets of Langerhans Hormones secreted directly into blood flow Alpha cell-glucagon Beta cell- insulin and amylin Delta cells- somatostatin gamma cells- pancreatic polypeptide Epsion cells- ghrelin Acinar cell synthesize, store, secrete digestive enzymes most active protein synthesizing cell in body
The Numbers 4th 5% 1.4% 1 of 76 33,370
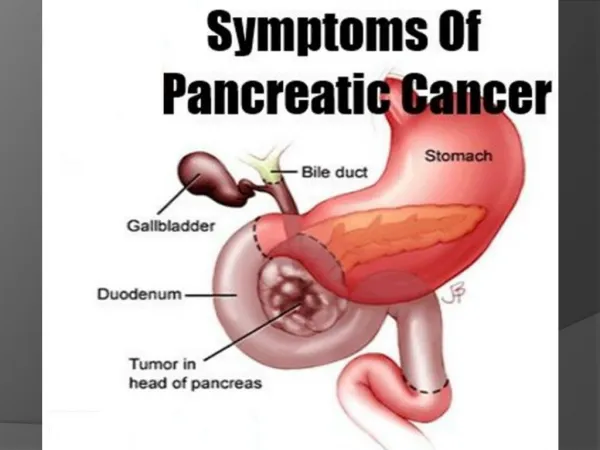
Pathophysiology • Location: • 80% head • 70% biliary obstruction • Local Invasion (most common) • Stomach, Duodenum, Colon, Portal or Superior Mesenteric Veins, Superior Mesenteric Artery • Distant Spread • Liver, Peritoneum, Lung • Desmoplastic lesions
Risk Factors • Family History • Smoking • Alcohol • Obesity • Diabetes mellitus • Chronic pancreatitis • Familial cancer syndromes
Serum CA 19-9 • Monosialoganglioside/glycolipid • Advantages: • Accessible • Relatively sensitive/ specific for pancreatic cancer • Levels correlate with: • tumor size • stage • Present uses: • Prognosis • Monitor disease progression
Therapy-Surgery Pancreaticoduodenectomy (Whipple procedure) Distal Pancreatectomy
Surgery and Survival Sener et al, J Am Coll Surg 1999;189(1):1-7.
Therapy • General Principles • MDC • Management of resectable disease • Surgery • Neoadjuvant • Controversial, may downstage disease • Adjuvant • Chemotherapy beneficial • Radiotherapy is controversial • Management of Locally advanced disease • Chemoradiotherapy downstages 30% to resectable • Management of metastatic disease • Gemcitabine –based combination treatments
Palliation-Pain • Celiac plexus neurolysis: • Anterior transgastric approach • CT or fluroscopy- percutaneous • Traverse bowel, further for needle to traverse, not real-time • EUS- through stomach • Stomach adjacent to celiac trunk, real-time • Posterior approach • CT or fluroscopy- percutaneous • Risk of paralysis (spinal arteries)
Palliation- Gastric Outlet Obstruction • Gastric Outlet Obstruction • Improved dietary performance (86%) • Comparison with surgery (2 studies) • Shorter time to oral intake • Shorter hospital stay • Complication rates • Endoscopic (0%) • Open (37.5%) • Laparoscopic (42.9%)
Introduction • Incidence 4/ 1 million population • Classification A (PNET) • Functional- clinical syndrome caused by hormone release • Non-functional • Classification B (NET) • Well-differentiated endocrine tumor • Benign behavior • Uncertain behavior • Poorly-differentiated endocrine tumor • Mixed exocrine-endocrine tumors
Introduction • Pathophysiology • Symptoms • inappropriate biologically active peptide release • Tumor mass effect • PET tumors also produce • Chromogranins (chromogranin A) • Alpha or Beta subunit of HCG • Peptides often released even in “non-functional” tumors that do not cause a clinical syndrome • Often multiple hormones released, but multiple tumor syndromes not common • Symptoms from hormones predate tumor symptoms
Tumor localization • Goals • Help localize for surgery • Detect multifocal tumors • i.e. gastrinomas • Detect metastatic disease • Avoidance of surgery
Case 1 • 44 YO white male weighing 325 pounds who became agitated, confused after awakening. He had accompanying palpitations, headache and sweating. He had elevated insulin and proinsulin levels while fasting and a fasting glucose <35. Computed tomography and Octreoscan were negative.
Insulinoma • Whipples triad (not specific) • Hypoglycemic symptoms • Blood sugar <50 • Symptom relief with glucose ingestion • Symptoms (fasting, exercise, missed meal) • Neurologic neuroglycopenia • Headache, confusion, lightheadedness, visual disturbance, irrational behavior, drowsiness, coma • Catecholemine release • Palpitations, tremor, sweating, irritability
Insulinoma • Characteristics • Most confined to pancreas • Solitary • Equal distribution in pancreas • Usually not malignant (10%) • Diagnosis • 72 hour fasting glucose and insulin test • Surgical cure rate 70-95%
Patient 2 • 41 YO male presented to clinic for a second opinion with watery bowel movements 5 times per day. He had mild diffuse abdominal discomfort, and had lost 20 pounds over the last year. He saw another gastroenterologist for this problem 3 years prior who did stool samples and a colonoscopy that was normal. He also had seen a naturopath.
Data • Gastrin: 470 • Chromogranin A: 2480 • Basal acid output 16.93 • Diarrhea resolved completely with PPI
Gastrinoma • Zollinger Ellison Syndrome- gastric acid hypersecretion due to release of gastrin from and endocrine neoplasm • Gastrin (gastric antrum): • Primary stimulant of post-prandial acid secretion • Trophic effect on gastric tissue (parietal cells) • Adult pancreas does not secrete gastrin
Gastrinoma • Symptoms: • Peptic ulcer disease • Duodenum 75% • Uncommon sites in small bowel • Diarrhea • Volume • Duodenal pH/ malabsorption • Gastroesophageal reflux • 66%
Gastrinoma • When to think of gastrinoma: • Duodenal ulcerations in unusual places • Diarrhea in a patients with idiopathic peptic ulcer disease/GERD • Patient with idiopathic peptic ulcer disease/GERD with history of hyperparathyroidism • Prominent gastric folds on UGI or endoscopy with idiopathic peptic ulcer disease/GERD or idiopathic diarrhea
Gastrinoma • Association • Sporadic (75%) • MEN-1 (25%) • 50% malignant • Duodenum most common extrapancreatic site
Gastrinoma • Fasting serum gastrin • 98% have elevated levels • 60% of ZES patients have mild to moderate elevation • Common differential: atrophic gastritis, PPI intake (look at gastric folds) • Gastric acid testing • Gastric pH <2 • BAO >10 meq/hour (94% of ZES patients) • Secretin injection test • Sensitivity 87-93%; specificity > 90% • Secretin promotes gastrin release in ZES • 2 μg/KG prompts rise >200 pg/ml
Patient 3 • SB is a 32 Y.O. female with abdominal distention and pain. She had an UGI that was mildly irregular at the duodenal sweep. CT showed a small hypervascular lesion in the neck of the pancreas c/w a NET. ACTH,calcitonin,gastrin, somatostatin,insulin and glucagon levels were normal. Calcium and CBC normal. Pancreatic polypeptide was 353 (normal <249). An EUS was performed.
Nonfunctioning Pancreatic Endocrine Tumors (PET) • Definition • PET with no clinical symptoms caused by hormone overproduction • May have elevated: • Pancreatic polypeptide • HCG • Chromogranin • Neurotensin • Usually: • Large (72%>5cm) • Malignant (64-92%) • Head
Nonfunctioning PET • Presentation • Most common • Abdominal pain (36%) • Jaundice (28%) • Incidental at surgery (16%) • Therapy • Rare diagnosis established prior to surgery • Survival • 44% at 5 years
Therapy • Localized Disease • Surgery • Enucleation, distal pancreatectomy, pancreaticoduodenectomy (Whipple procedure) • Tumor type influences surgery • Observation • Non-functioning tumors <2cm • Hepatic Metastasis • Surgery • resection • transplantation • Hepatic artery embolization • Radiofrequency ablation/ cryoablation • Chemotherapy (rapidly growing or poorly differentiated)
Summary • Pancreatic cancer can be exocrine or endocrine in nature. • Pancreatic adenocarcinoma (exocrine) is most common. • The 5-year survival for pancreatic adenocarcinoma (5%) is much worse than for PNET’s. • Pancreatic neuroendocrine tumors (endocrine) can cause symptoms from secreted biologically active peptides or from tumor effect • Surgery is the only curative therapy for pancreatic cancer, but may not be needed in small non-functional pancreatic neuroendocrine tumors