Download
1 / 35
350 likes | 515 Views
Susan dosReis, PhD, Edward Knapp, PhD, Ming- Hui Tai, Bpharm , MS Department of Pharmaceutical Health Services Research University of Maryland School of Pharmacy, Baltimore, MD.

E N D
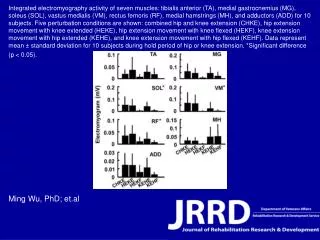
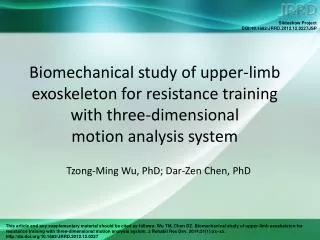
Susan dosReis, PhD, Edward Knapp, PhD, Ming-Hui Tai, Bpharm, MS Department of Pharmaceutical Health Services Research University of Maryland School of Pharmacy, Baltimore, MD Psychotropic Treatment of Children in Foster Care: From Clinical Practice to Practical Monitoring and Future Directions
Learning Objectives • To identify the major therapeutic classes of psychotropic medications and the indications for use in children and adolescents; • To identify key public concerns, legislation, and scientific reports about psychotropic prescribing to youth in foster care; • To recognize factors related to variability in psychotropic medication use and outcomes for youth in foster care.
Overview of the Workshop • Part 1: Review major therapeutic classes, the clinical evidence, and the place in therapy for pediatric use of psychotropic medications • Part 2: Present key court cases, media attention, and legislative initiatives that have heightened public concern • Part 3: Present some empirical research from national surveys of states’ psychotropic monitoring programs and localized data on patterns, outcomes, and early childhood trajectories. • Wrap-up: Discuss implications and future directions
What defines a psychotropic medication? A psychotropic medication is a medication that is used to treat the symptoms of mental disorders such as schizophrenia, depression, bipolar disorder (sometimes called manic-depressive illness), anxiety disorders, and attention deficit-hyperactivity disorder (ADHD). National Institute of Mental Health A psychotropic medication is “any medication capable of affecting mind, emotions, and behavior” that is used for “antipsychotic, antidepressant, antimanic, antianxiety, behavioral modification, or behavioral management purposes.” Definition adapted from Ill. Admin code tit. 89 IIIb pt. 325.20 {2012}
Major Psychotropic Medication Classes • There are generally 6 major therapeutic classes of psychotropic medications that are prescribed for pediatric patients. • ADHD medications • Antidepressant • Antipsychotic • Mood stabilizer (lithium and anticonvulsants) • Sedative/hypnotic • Anxiolytic • Alpha-agonists also are prescribed frequently in psychiatric practice, although this is not a psychotropic medication. • Clonidine and guanfacine used for behavior management Adapted from Texas Department of Family and Protective Services “Psychotropic Medication Utilization Parameters for Children and Youth in Foster Care”, September 2013. Available from: http://www.dpfs.state.tx.us/Child_Protection/Medical_Services/guide-psychotropic.asp
Clinical Guidelines for Psychotropic Medication Use in Children and Adolescents • American Academy of Child and Adolescent Psychiatry (AACAP) Guidelines • Initiation of psychotropic medication • Role of psychosocial treatments • Recommendations for polypharmacy • Recommendations for monitoring
Clinical Guidelines for Psychotropic Medication Use in Children and Adolescents • Using Medication Treatment • Three phases of treatment • Acute – initiation and dose adjustments to maximize benefit • Maintenance – remission or recovery occurs • Discontinuation – medication is tapered Practice Parameters on the Use of Psychotropic Medication in Children and Adolescents. J. AmerAcad Child Adolesc Psychiatry. 2009; 48: 961-973.
Clinical Guidelines for Psychotropic Medication Use in Children and Adolescents • Role of Psychosocial Treatment • Medication may be started before, concurrent with or after psychosocial treatments. • When behavior precludes involvement in psychosocial treatment, a medication is often started before or concurrently. • Scarcity of trained providers to deliver psychosocial treatments, and so medication may be the only evidence-based option. Practice Parameters on the Use of Psychotropic Medication in Children and Adolescents. J. AmerAcad Child Adolesc Psychiatry. 2009; 48: 961-973.
Clinical Guidelines for Psychotropic Medication Use in Children and Adolescents • Recommendations for Monitoring • Several factors determine monitoring frequency: • Type of medication, the risk for side effects, patient need for psychological support, risk for non-adherence, phase of treatment. • Monitoring visits vary by treatment phase: • May be more frequent during the acute and discontinuation phases • Less frequent during the maintenance phase, provided good stable response to therapy • No clear guidelines for how long to monitor after discontinuation Practice Parameters on the Use of Psychotropic Medication in Children and Adolescents. J. AmerAcad Child Adolesc Psychiatry. 2009; 48: 961-973.
Clinical Guidelines for Psychotropic Medication Use in Children and Adolescents • Recommendations for Polypharmacy • Treatment/monitoring plan, patient/family education, assent/consent, and trial basis should be implemented before initiation of medication combinations. • Rationale for medication combinations: • Treat multiple conditions • Add on/augmentation • Manage side effects • Limited evidence to support medication combinations Practice Parameters on the Use of Psychotropic Medication in Children and Adolescents. J. AmerAcad Child Adolesc Psychiatry. 2009; 48: 961-973.
Clinical Evidence of Efficacy in the Management of Pediatric Mental Illness • Disruptive behavior disorders • ADHD • Internalizing disorders • Depression • Anxiety • Mood disorders • Bipolar • Mood dysregulation • Psychosis and schizophrenia • Developmental Disabilities • Autism • Tourette’s • Other • Irritability
Clinical Efficacy for the Management of Pediatric Attention-Deficit/Hyperactivity Disorder (ADHD) • Multi-modal Treatment of ADHD Study (MTA) • Children aged 7-9 years old were randomized to one of 4 treatment groups • Medication management (MedMgt) • Behavioral treatment (Behav) • Combined treatment (Comb) • Community care (CCare) • 14-month study • Established the efficacy of medication management over other interventions for ADHD symptoms The MTA Cooperative Group. Archives of General Psychiatry. 1999; 56:1073-1086.
Clinical Efficacy for the Management of Pediatric Anxiety • Child-adolescent Anxiety Multimodal Study (CAMS) • 488 children and adolescents aged 7-17 years old • Separation or generalized anxiety disorder or social phobia • Moderate to severe anxiety and impairment • Randomized to one of four treatment arms: • Sertraline (SSRI) CBT (cognitive behavioral therapy) • Sertraline + CBT Placebo NEJM. 2008; 359:2753-2766.
Clinical Efficacy for the Management of Pediatric Depression Treatment for Adolescents with Depression (TADS) • 439 adolescents aged 12-17 years old with a DSM-IV diagnosis of major depressive disorder (MDD) Fluoxetine, Cognitive-Behavioral Therapy, and Their Combination for Adolescents with Depression. Treatment for Adolescents with Depression Study (TADS) Randomized Controlled Trial. JAMA. 2004; 292:807-820
Timeline of Court Cases and Reports Related to Psychotropic Use Among Foster Youth 2009Suicide of 7 y.o. Gabriel Myers, a Florida youth in foster care on multiple psychotropic medications B.H. v Suter: ACLU class action lawsuit against Illinois DCFS State Advocacy Council releases reports on psychotropic medication use among Florida youth in foster care Texas State Comptroller releases “Forgotten Children” report on Texas foster care Report on Nevada foster care deaths 2001-2004 ‘Henry A.’ class-action lawsuit against Clark County, NV Child Welfare Services 1988 2002-2003 2004 2005 2010 2009
Emergence of Research Publications on Psychotropic Medication Use Among Youth in Foster Care 2001 - dosReis et al. Access to mental health services, diagnoses, and psychotropic use for disabled youth and youth in foster care 2008 – Zito et al. Study psychotropic patterns in foster care youth in Texas 2010 – MMDLN 16-state survey compares psychotropic use in Medicaid-eligible youth 2004 and 2007. 2012 – Rubin et al. 47-state Medicaid study of psychotropic use in foster care children 2002 - 2008 2012 – Walsh & Mattingly. NSCAW II rural vs urban psychotropic use in children in child welfare 1999 – Zima et al. Psychotropic medication treatment among children in foster care 2006 – Constantine & Tandon study Florida pediatric antipsychotic use 1998 2000 2002 2004 2006 2008 2010 2012
Emergence of Clinical Guidelines for Psychotropic Medication Use in Children 2008 – Casey Foundation releases child welfare mental health guidelines 2003 – WHO releases recommendations for treating pediatric mental disorders 2009 – AACAP guidelines for pediatric psychotropic use 2006 – APA working group report on psychotropic medications in children & adolescents 2011- AACAP guidelines for anti-psychotic use in children and adolescents 1998 2000 2002 2004 2006 2008 2010 2012
Federal Response to Psychotropic Medication Use Among Youth in Foster Care 2011 – Child and Family Services Improvement and Innovation Act passed 2011 – Senate sub-committee hearings on psychotropic medication policy and foster care children 2011 – GAO report recommends HHS guidelines for psychotropic prescribing and monitoring 2011 - DHHS announces collaboration between CMS, ACF, and SAMHSA to promote monitoring and systemic approaches to regulating psychotropic medication use in foster care children 2012-13 – CMS releases guides to informational resources and state approaches to DURs 1991 1992 1995 2000 2004 2005 2006 2008 2009 2010 2011 2012 2013
Public Health Concern about Psychotropic Medications Use Among Foster Children • Psychotropic medications have been efficacious in treating mental illness • Evidence for effectiveness in children is lacking • Side effect profile ranges from mild to serious, and the long-term safety is essentially unknown GAO Report on Foster Children: Oversight of Psychotropic Prescriptions. Report #: GAO-12-201. 2011
Public Health Concern about Psychotropic Medications Use Among Foster Children • Children in foster care tend to have more serious mental illness and typically receive more psychotropic medications • Children in foster care receive health care coverage through Medicaid, and thus several agencies are involved in the oversight and management of youth in foster care GAO Report on Foster Children: Oversight of Psychotropic Prescriptions. Report #: GAO-12-201. 2011
Government Accountability Office (GAO) Report • Government Accountability Office (GAO) prepared a report of psychotropic medication use among children in foster care. • Goals: To examine psychotropic use with respect to: • Foster and non-foster children in Medicaid in 2008, including indicators of potential health risks • Health Risks: 5+ medications; prescriptions exceeding dosing guidelines; medication use under 1 year of age • Federal/state oversight policies in effect for foster children GAO Report on Foster Children: Oversight of Psychotropic Prescriptions. Report #: GAO-12-201. 2011
GAO Report Findings • Psychotropic use was 3-5 times higher in foster compared with non-foster children • Factors contributing to the higher rates • Exposure to trauma • Frequency of changes in foster placement • Varying oversight policies • Foster children have higher rates of health risk factors • States’ psychotropic monitoring programs fall short of best practice guidelines GAO Report on Foster Children: Oversight of Psychotropic Prescriptions. Report #: GAO-12-201. 2011
GAO Recommendations • Secretary of Health and Human Services (HHS) should offer guidance to state Medicaid and child welfare agencies on best practices for monitoring psychotropic use among children in foster care • Guidance would address: • Informed consent • Oversight • Consultation • Information sharing • Administration for Children and Families (ACF) disseminated information to states in 2012 summit GAO Report on Foster Children: Oversight of Psychotropic Prescriptions. Report #: GAO-12-201. 2011
Part 3: Empirical Research on Psychotropic Use in Foster Care
National Perspective on Psychotropic Medications for Youth in Foster Care Interstate Variation
National Variation Psychotropic Medication Use Among Medicaid-enrolled Foster Care Youth • Medicaid data from 47 states and the District of Columbia for 2002-2007 • Over 600,000 children annually aged 3-18 years old • Main outcomes: • Prevalence of filled prescriptions for antipsychotics • Psychotropic polypharmacy (≥3 psychotropic classes) • Stratified by age group: • 3-5 years old • 6-11 years old • 12-18 years old Rubin, D. et al. Interstate variation in trends of psychotropic medication use among Medicaid-enrolled children in foster care. Child and Youth Services Review. 2012; 34:1492-99.
National Variation Psychotropic Medication Use Among Medicaid-enrolled Foster Care Youth Rubin, D. et al. Interstate variation in trends of psychotropic medication use among Medicaid-enrolled children in foster care. Child and Youth Services Review. 2012; 34:1492-99.
National Variation Psychotropic Medication Use Among Medicaid-enrolled Foster Care Youth Rubin, D. et al. Interstate variation in trends of psychotropic medication use among Medicaid-enrolled children in foster care. Child and Youth Services Review. 2012; 34:1492-99.
National Variation Psychotropic Medication Use Among Medicaid-enrolled Foster Care Youth Rubin, D. et al. Interstate variation in trends of psychotropic medication use among Medicaid-enrolled children in foster care. Child and Youth Services Review. 2012; 34:1492-99.
National Variation Psychotropic Medication Use Among Medicaid-enrolled Foster Care Youth Rubin, D. et al. Interstate variation in trends of psychotropic medication use among Medicaid-enrolled children in foster care. Child and Youth Services Review. 2012; 34:1492-99.
Summary • Youth in foster care have behavioral and emotional problems that are clinically challenging to manage. • Emergence of clinical cases precedes public action. • Only recently have programs been implemented for statewide oversight and monitoring of psychotropic treatment and the outcomes have not been evaluated. • Antipsychotic medications have increased in use while other therapeutic classes have remained stable. • Use starts young and becomes more persistent over time. • An agenda for advocacy in professional and public health arenas is needed to establish benchmarks for psychotropic medication use as well as clinical and functional improvement and placement stability.
References March J, Silva S, Petrycki S, Curry J, Wells K, Fairbank J, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial. JAMA. 2004;292(7):807-20. Practice Parameters on the Use of Psychotropic Medication in Children and Adolescents. J. AmerAcad Child Adolesc Psychiatry. 2009; 48:961-973. “Psychotropic Medication Utilization Parameters for Children and Youth in Foster Care”, September 2013. Available from: http://www.dpfs.state.tx.us/Child_Protection/Medical_Services/guide-psychotropic.asp Rubin D, Matone M, Huang YS, dosReis S, Feudtner C, Localio R. Interstate variation in trends of psychotropic medication use among Medicaid-enrolled children in foster care. Child and Youth Services Review. 2012;34:1492-9. The MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry. 1999;56:1073-86. US Government Accountability Office. Foster Children: HHS Guidance Could Help States Improve Oversight of Psychotropic Prescriptions. 2011 Contract No.: GAO-12-201. US Government Accountability Office. Children's Mental Health: Concerns Remain about Appropriate Services for Children in Medicaid and Foster Care. 2012 Contract No.: GAO-13-15. Walkup JT, Albano AM, Piacentini J, Birmaher B, Compton SN, Sherrill JT, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. New England Journal of Medicine. 2008;359(26):2753-66.
Acknowledgements • Dr. Gloria Reeves, MD • Terry Shaw, PhD • Zhongyuan Zhou and Donnetta McFadden-Coleman