Download
1 / 1
10 likes | 105 Views
State Legislation Expanding the Role of Nurse Practitioners in a Workers’ Compensation System: Effects on Disability and Costs. Jeanne M. Sears, PhC, MS, RN, Department of Health Services Thomas M. Wickizer, PhD, MPH, D epartment of Health Services

E N D
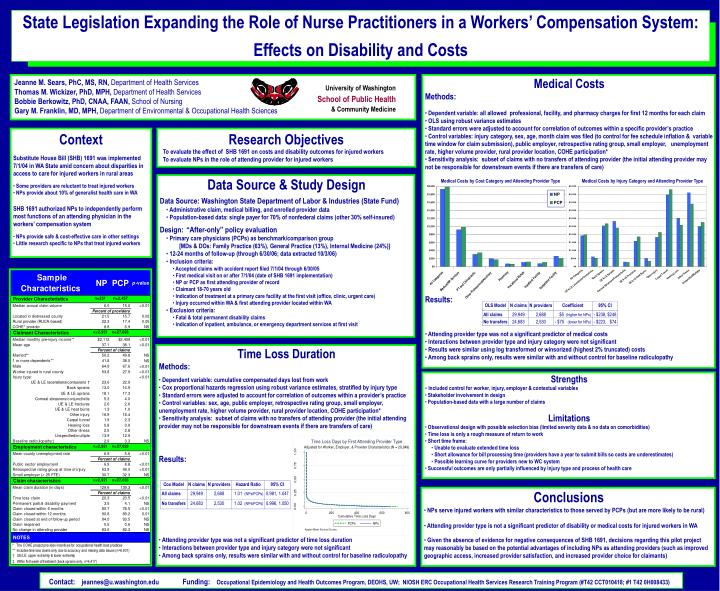
State Legislation Expanding the Role of Nurse Practitioners in a Workers’ Compensation System: Effects on Disability and Costs Jeanne M. Sears, PhC, MS, RN, Department of Health Services Thomas M. Wickizer, PhD, MPH, Department of Health Services Bobbie Berkowitz, PhD, CNAA, FAAN, School of Nursing Gary M. Franklin, MD, MPH, Department of Environmental & Occupational Health Sciences • Medical Costs • Methods: • Dependent variable: all allowed professional, facility, and pharmacy charges for first 12 months for each claim • OLS using robust variance estimates • Standard errors were adjusted to account for correlation of outcomes within a specific provider’s practice • Control variables: injury category, sex, age, month claim was filed (to control for fee schedule inflation & variable time window for claim submission), public employer, retrospective rating group, small employer, unemployment rate, higher volume provider,rural provider location, COHE participation* • Sensitivity analysis: subset of claims with no transfers of attending provider (the initial attending provider may not be responsible for downstream events if there are transfers of care) • Results: • Attending provider type was not a significant predictor of medical costs • Interactions between provider type and injury category were not significant • Results were similar using log transformed or winsorized (highest 2% truncated) costs • Among back sprains only, results were similar with and without control for baseline radiculopathy University of Washington School of Public Health & Community Medicine • Context • Substitute House Bill (SHB) 1691 was implemented 7/1/04 in WA State amid concern about disparities in access to care for injured workers in rural areas • Some providers are reluctant to treat injured workers • NPs provide about 10% of generalist health care in WA • SHB 1691 authorized NPs to independently perform most functions of an attending physician in the workers’ compensation system • NPs provide safe & cost-effective care in other settings • Little research specific to NPs that treat injured workers Research Objectives To evaluate the effect of SHB 1691 on costs and disability outcomes for injured workers To evaluate NPs in the role of attending provider for injured workers • Data Source & Study Design • Data Source: Washington State Department of Labor & Industries (State Fund) • Administrative claim, medical billing, and enrolled provider data • Population-based data: single payer for 70% of nonfederal claims (other 30% self-insured) • Design:“After-only” policy evaluation • Primary care physicians (PCPs) as benchmark/comparison group • [MDs & DOs: Family Practice (63%), General Practice (13%), Internal Medicine (24%)] • 12-24 months of follow-up (through 6/30/06; data extracted 10/3/06) • Inclusion criteria: • Accepted claims with accident report filed 7/1/04 through 6/30/05 • First medical visit on or after 7/1/04 (date of SHB 1691 implementation) • NP or PCP as first attending provider of record • Claimant 18-70 years old • Indication of treatment at a primary care facility at the first visit (office, clinic, urgent care) • Injury occurred within WA & first attending provider located within WA • Exclusion criteria: • Fatal & total permanent disability claims • Indication of inpatient, ambulance, or emergency department services at first visit Medical Costs by Cost Category and Attending Provider Type Medical Costs by Injury Category and Attending Provider Type • Time Loss Duration • Methods: • Dependent variable: cumulative compensated days lost from work • Cox proportional hazards regression using robust variance estimates, stratified by injury type • Standard errors were adjusted to account for correlation of outcomes within a provider’s practice • Control variables: sex, age, public employer, retrospective rating group, small employer, unemployment rate, higher volume provider, rural provider location, COHE participation* • Sensitivity analysis: subset of claims with no transfers of attending provider (the initial attending provider may not be responsible for downstream events if there are transfers of care) • Results: • Attending provider type was not a significant predictor of time loss duration • Interactions between provider type and injury category were not significant • Among back sprains only, results were similar with and without control for baseline radiculopathy • Strengths • Included control for worker, injury, employer & contextual variables • Stakeholder involvement in design • Population-based data with a large number of claims • Limitations • Observational design with possible selection bias (limited severity data & no data on comorbidities) • Time loss is only a rough measure of return to work • Short time frame: • Unable to evaluate extended time loss • Short allowance for bill processing time (providers have a year to submit bills so costs are underestimates) • Possible learning curve for providers new to WC system • Successful outcomes are only partially influenced by injury type and process of health care • Conclusions • NPs serve injured workers with similar characteristics to those served by PCPs (but are more likely to be rural) • Attending provider type is not a significant predictor of disability or medical costs for injured workers in WA • Given the absence of evidence for negative consequences of SHB 1691, decisions regarding this pilot project may reasonably be based on the potential advantages of including NPs as attending providers (such as improved geographic access, increased provider satisfaction, and increased provider choice for claimants) Contact: jeannes@u.washington.eduFunding:Occupational Epidemiology and Health Outcomes Program, DEOHS, UW; NIOSH ERC Occupational Health Services Research Training Program (#T42 CCT010418; #1 T42 0H008433)