Download
1 / 28
380 likes | 672 Views
Lynch Syndrome and Colorectal Cancer. Steven G. Proshan , M.D. Annapolis Colon and Rectal Surgeons Anne Arundel Medical Center November 8, 2014. Lynch Syndrome (LS). Familial Predisposition to Colorectal and other cancers Autosomal Dominant Henry Lynch, MD 1966

E N D
Lynch Syndrome and Colorectal Cancer Steven G. Proshan, M.D. Annapolis Colon and Rectal Surgeons Anne Arundel Medical Center November 8, 2014
Lynch Syndrome (LS) Familial Predisposition to Colorectal and other cancers Autosomal Dominant Henry Lynch, MD 1966 Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Colorectal Cancer in LS Cancers more frequently Cancers at younger age (40’s) Right sided cancers Adenoma to carcinoma sequence more rapid Synchronous and Metachronous Cancers Lifetime Risk 10-74% (vs. 5.5% without) Better Prognosis
Genetics of CRC Sporadic (65%–85%) Familial (10%–30%) Rare CRC syndromes (<0.1%) Lynch syndrome (3%) MYH associated polyposis (MAP) (1%) Familial adenomatous polyposis (FAP) (1%)
A Classic HNPCC/Lynch Family CRC dx 50s CRC dx 45 CRC dx 61 CRC dx 75 OvarianCa, dx 64 CRC dx 48 CRC dx 52 EndometrialCa, dx 59 45 CRC dx 42
Clinical Diagnosis of LSAmsterdam I Criteria (1991) 1. Three or more relatives with histologically verified colorectal cancer, 1 of which is a first-degree relative of the other two. Familial adenomatous polyposis should be excluded. 2. Two or more generations with colorectal cancer. 3. One or more colorectal cancer cases diagnosed before the age of 50 years.
Clinical Diagnosis of LSAmsterdam II Criteria (1999) 1. Three or more relatives with histologically verified HNPCC-associated cancer (colorectal cancer, cancer of the endometrium, small bowel, ureter, or renal pelvis), 1 of which is a first-degree relative of the other 2. Familial adenomatous polyposis should be excluded. 2. Cancer involving at least 2 generations. 3. One or more cancer cases diagnosed before the age of 50 years.
Clinical Diagnosis of LSRevised Bathesda Guidelines (2004) 1. CRC diagnosed at younger than 50 years. 2. Presence of synchronous or metachronous CRC or other LS-associated tumors.* 3. CRC with MSI-high pathologic-associated features (Crohn-like lymphocytic reaction, mucinous/signet cell differentiation, or medullary growth pattern) diagnosed in an individual younger than 60 years old. 4. Patient with CRC and CRC or LS-associated tumor* diagnosed in at least 1 first-degree relative younger than 50 years old. 5. Patient with CRC and CRC or LS-associated tumor* at any age in 2 first-degree or second-degree relatives. * LS-associated tumors include tumor of the colorectum, endometrium, stomach, ovary, pancreas, ureter, renal pelvis, biliary tract, brain, small bowel, sebaceous glands, and kerotoacanthomas.
LS Genetic Alterations • Microsatellite Instability (MSI) • MSI - High • MSI - Low • MS - Stable • MSI – High Better Prognosis • Most MSI Colorectal Cancers are not LS (12% of sporadic CRC)
Microsatellite Instability Normal Cells -CG- -CGCGCGCG -CG- -CGCGCGCG -CG -CGCGCGCG- -CG- -CGCGCGCG Normal Microsatellites Tumor Cells -CG- -CG- -CG- -CGCG- -CGCGCG- -CGCGCGCGCG- -CGCGCGCGCG- -CGCGCG- -CG- -CGCG- Microsatellite Instability
Mismatch Repair (MMR) Genes and Proteins Proofread Replicated DNA Problem will be most obvious in repetitive sequences Defect in both copies leads to cancer If already carries one defect, at high risk to develop a second defect – Lynch Syndrome LS is Autosomal Dominant
Aa aa aa aa Aa Aa Carrier Carrier Non-carrier Non-carrier 1/2 1/2 Autosomal Dominant Inheritance Carrier Parent Non-carrier Parent
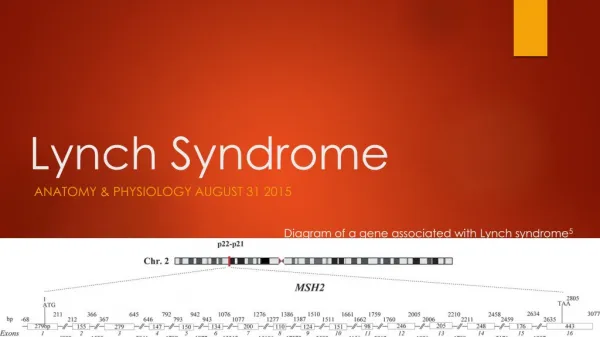
Mismatch Repair (MMR) Genes MLH1 MSH2 MSH6 PMS2 EPCAM (Promotor for MSH2)
MSH2 MSH6 MLH1 PMS2
Universal Tumor Testing for LS • MSI Testing • Inexpensive • Prognostic and Treatment Information • MMR Protein Testing • Inexpensive • Directs which gene to look at • Confirm Positive Results with Gene Analysis
Followup Genetic Counseling Gene Testing Appropriate Family Members Familial Colorectal Cancer Type X (FCRCTX)
Treatment of Colon Cancer in LS Patients • Partial Colectomy • Risk of Metachronous Cancer 16-19% at 10 years • Total or Subtotal Colectomy with Ileorectal/Ileosigmoid Anastomosis • Risk of Metachronous Cancer 0-3.4% at 10 years • Diarrhea • Need to consider age and sphincter function
Treatment of Rectal Cancer in LS Patients • Resection of Rectum with Anastomosis • Risk of Metachronous Cancer 69% at 30 years with colonoscopy every 1.6 years • Total Proctocolectomy with Ileal Pouch-Anal Anastomosis (IPAA) • Standard of Care for cancer with UC or FAP • LS patients older • Total Proctocolectomy with End Ileostomy
CRC Screening in LS Patients Colonoscopy every 1-3 years leads to fewer CRC and at a later age than unscreened Colonoscopy every 1-3 years leads to similar CRC mortality compared to those without LS, although more CRC diagnosed More frequent colonoscopy (≤ 2 years) better
CRC Screening in LS Patients Guideline: Screening for CRC by colonoscopy is recommended in persons at risk (first-degree relatives of those affected) or affected with LS every 1 to 2 years, beginning between ages 20−25 years or 2−5 years before the youngest age of diagnosis of CRC in the family if diagnosed before age 25 years. May need to adjust based on exact family history and which gene is mutated.
Endometrial Cancer in LS Second most common cancer 75% Stage I and 88% 5 year survival Hard to prove screening helps Annual Pelvic Exam and Endometrial Sampling Offered Starting at Age 30-35
Ovarian Cancer in LS No data as to screening Transvaginal Ultrasound and CA-125 Screening does not seem to help with BRCA1 and BRCA2 patients Annual Transvaginal Ultrasound Offered Starting at Age 30-35
Prophylactic Hysterectomy and Oophorectomy in LS • Retrospective analysis of 315 women with MMR mutations • 33% Uterine cancer without surgery • No uterine cancer with surgery • 5.5% Ovarian cancer without surgery • No ovarian cancer with surgery • Guideline: Hysterectomy and Oophorectomy after childbearing or at age 40
Gastric Cancer in LS Lifetime Risk 0.2-13% EGD every 2-3 years beginning age 30-35 Treat H.pylori if found Modify based on family history and gene mutation
Urinary Cancers in LS Not much data screening (urinalysis, urine cytology) helps Inexpensive Noninvasive Easy Consider annually starting age 30-35
Other Cancers in LS • No screening or no increased screening beyond that for usual population • Pancreatic • Small Intestine • Prostate • Breast • Either no clear increased risk or no good screening test