Download
1 / 23
240 likes | 546 Views
Infective Endocarditis A Disease in Disguise. Optimizing Recognition &Response Ann Krinks Trainee Advanced Nurse Practitioner. Raise Awareness of Infective Endocarditis by Launching an Educational Awareness Campaign.

E N D
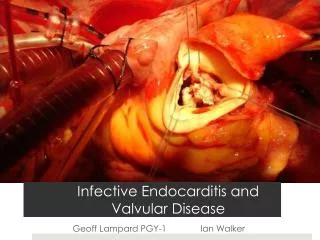
Infective Endocarditis A Disease in Disguise Optimizing Recognition &Response Ann Krinks Trainee Advanced Nurse Practitioner
Raise Awareness of Infective Endocarditis by Launching an Educational Awareness Campaign • Promote awareness of infective endocarditis throughout the health care setting • Alert health care professionals to the seriousness of the disease challenging them to recognise and act upon presenting signs & symptoms • To be aware of high risk patients who may be susceptible to developing infective endocarditis • To get health care professional to think past initial diagnosis and consider IE as the primary cause of underlying conditions
Impact on Practice • Raise the bar on quality of care • Improve patient safety • Early recognition of signs & symptoms • Early diagnosis • Early treatment • Improved prognosis and patient outcome
A deadly disease, high mortality nearly 100% if not recognised or left untreated & 20-25% when treated. • Historically associated with heart valve damage from rheumatic fever (now un-common in the developed world). • Perceived to be uncommon & diagnosis is often missed or diagnosed late when the disease is advanced • Despite evolution in antibiotic therapy & sepsis prevention , incidence not declined in last 30 years ? • Changes in nature of disease & emergence of new causes – degenerative heart disease in the growing elderly population has replaced rheumatic fever as the major cause of valveular disease
Why? • Difficult to diagnose – no single clinical sign or symptom & no single diagnostic front line test • Many cases missed or diagnosed late when disease is advanced • Antibiotic resistance ( makes treatment challenging) • Disease in disguise- can manifest with varied clinical presentations • Symptoms can be non specific – viral symptoms, lethargy, low grade fever (25% of patients take over 1/12 to be admitted after onset of initial symptoms)
Microbial infection of the endothelial surface of the heart & heart valves Caused by micro-organisms , usually bacteria, also fungi causing inflammation within the endocardium (inner lining of the heart) Micro-organisms can adhere & multiply on the heart valves leading to vegetation growth (clumps of bacteria red & white blood cells, fibrin) Vegetation can break off & cause emboli to occlude blood vessels within the body ( a serious complication of IE)
Bacteria enter the bloodstream causing bacteraemia Bacteria can settle on normal or abnormal heart valves This can damage or destroy the heart valves( leading to valve perforation)
Staphylococcus aureus (nose, skin, respiratory tract) Staphylococcus epidermidis (normal skin flora, immunocompromised. …patients, hospital acquired)
Streptococci viridans (mouth) Enterococci (normal intestinal flora)
Fungal Endocarditis On mitral valve Candida Albicans ( oral & genital infections)
Who's at Risk? • Prosthetic valves • Degenerative heart valve disease • Congenital heart defects (patent ductus arteriosus, VSD) • Implanted cardiac devices Pacemaker, ICD • Long term indwelling vascular catheters Hickman lines, PICC lines • Immunocompromised • Injection drug users • Risky social behaviour eg Body piercings, Tattoos • Previous endocarditis
Presentation Initially symptoms may be vague & put down to viral illness • Low grade fever • Chills • Night sweats • Fatigue • Arthralgia • Weight loss 85% patients present with a new or worsening existing murmur
Cardiac signs- resulting from damaged valves • New heart murmur • Change in existing murmur • ↓ Cardiac output (valve perforation) • Heart Failure • Conduction disorders (mainly) AV blocks • Myocardial infarction (coronary embolism)
Dermatological signs – result of small emboli travelling to peripheral vessels Splinter haemorrhage Oslers nodes (painful nodules on fingers & toes)
Janeway lesions (Painless lesions on palms & soles …of feet) Nail fold infarct ( Systemic emboli)
Petechiae Inside eyelids Oral mucosa
Petechial rash (non –blanching ) Roth spots (retinal haemorrhage seen on fundoscopy)
Complications of embolization Symptoms will depend on where the emboli dislodge and where they go RIGHT SIDE - Tricuspid PULMONARY CIRCULATION PE LUNG ABCESS LEFT SIDE- Mitral BRAIN (stroke) KIDNEY SPLEEN (infarct) MI
Management • Early recognition • Early blood cultures ( ideally pre antibiotic) to avoid false negative results • Early echo TTE (inadequate views in up to 20%) /TOE (>90% sensitivity detects small emboli <5mm) • Team approach involve Cardiologist, ID, Microbiologist • Treatment is with lengthy IV antibiotic therapy +/- surgery
Key Message • Infective endocarditis is a diverse disease and can masquerade as other illnesses • Vigilance & suspicion are key • Suspect IE in fever of unknown origin • FEVER + MURMUR INFECTIVE ENDOCARDITIS (until proven otherwise) ENDOCARDITIS THINK?