Download

1 / 50
500 likes | 727 Views
PENGENDALIAN IBU HAMIL SIFILIS POSITIF. Dr. Nor Azah bt Mohamad Nawi Pakar Perubatan Keluarga UD54 Klinik Kesihatan Bakar Arang. KANDUNGAN. Apakah VDRL, RPR, TPHA dan TPPA? Syphilis – klasifikasi dan rawatan Pengurusan kontak MSA untuk ulser genital. VDRL dan RPR.

E N D
PENGENDALIAN IBU HAMIL SIFILIS POSITIF Dr. Nor AzahbtMohamadNawi PakarPerubatanKeluarga UD54 KlinikKesihatanBakarArang
KANDUNGAN • Apakah VDRL, RPR, TPHA dan TPPA? • Syphilis – klasifikasidanrawatan • Pengurusankontak • MSA untukulser genital
VDRL dan RPR • Venereal Diseases Research Laboratory • Jugadikenalisebagai non-treponemal test. • RPR: Rapid Plasma Reagin • Ujiansaringanuntuksifilis. • False positive: kehamilan, yaws, malaria, Connective tissue disease, HIV, leprosy etc. • Untukdiagnossebagaisifilis, perlusahkandgnujianpengesahan: • TPHA, TPPA, dark-ground microscopy, FTA-Abs, ELISA, EIA, atau PCR.
Diagnosis • Dark ground field microscopy: Treponema pallidum sphirochaette 2. Serum VDRL 3. Serum TPHA 4. FTA abs
TPHA/TPPA? • TPHA: Treponemapallidumhamagglutination assay • Bound to erthrocytes • TPPA: Treponemapallidum particle agglutination • Bound to gelatin • Barudanlebihmudahdari TPHA • Kedua-2 mengesanantibodi, • Dilakukanbila RPR/VDRL reactive
InterpretasiUjianDarah SEJARAH PENDEDAHAN PENYAKIT PENTING
Syphilis Cause: Treponemapallidum A sphirochaette 50% pesakitada tanda-2 klasikal Screening : at booking and 28/52 POA. Cara Jangkitan: Diperolehi/Acquired Early Late Kongenital Early, < 2 years Late, > 2 years
Natural history of syphilis (Course of untreated syphilis) Spontaneous cure (30%) Primary syphilis Exposure Secondary syphilis Early latent Late latent syphilis(30%) Neuro- syphilis (12%) Cardio vascular (14%) Gumma (14%)
Acquired Syphilis Early Syphilis: 1st 2 years Late Syphilis: After 2 years Late Latent - Tiadagejala Tertiary Benign 1 – 45 (15) years later Benign gumma of skin, bones 3. Cardiovascular 15 – 30 years later Aortic aneurysm 4. Neurosyphilis - Bila-bilamasa Berlakulebihawaldikalangan RVD positive • Primary • IP 9 – 90 days • Chancre (ulcer) and lympadenopathy 2. Secondary: stage bacteraemia • IP: 6 wk – 6/12 • Generalised non-irritating skin lesion, condylomatalata , mucocutaneous lesion and patchy alopecia 3. Early latent: Positive serology without Sn n Sx
TYPES OF GENITAL ULCERS
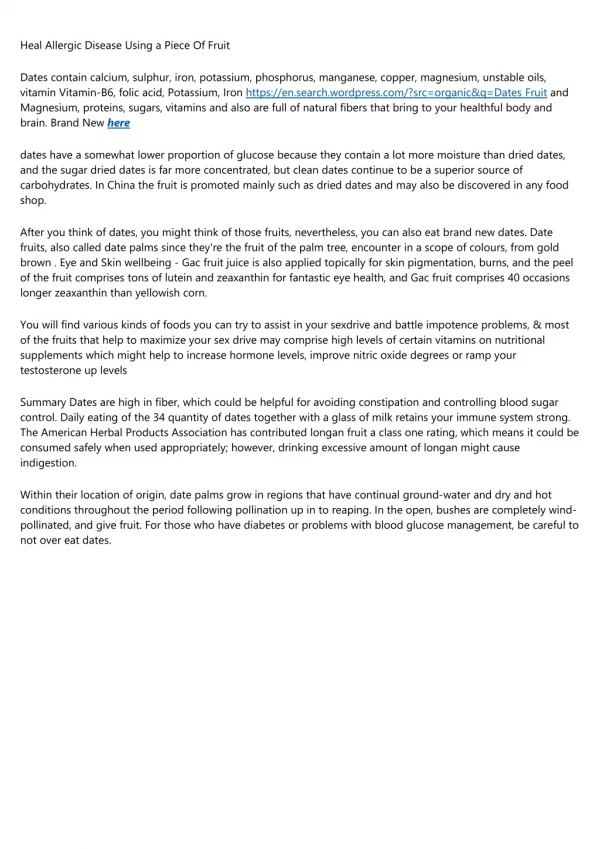
Early : Primary syphilis IP: 1-3 weeks Usually Painless single papule then became ulcer, round/oval Well circumscribed, clean floor, no exudate Usually no vesicle Regional lymphadenopathy Any anogenital ulcer should be considered to be due to syphilis unless proven otherwise. 90% genital ulcer, 10% extragenital
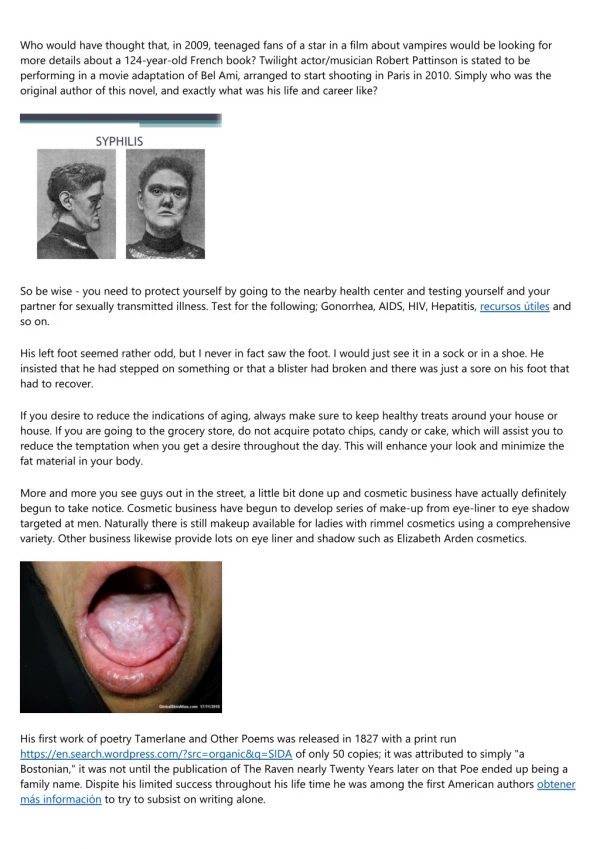
Primary syphilis (9 – 90 days) Chancre
Early: Secondary syphilis • 6 weeks to 6 months • Stage of bacteremia • May cause uveitis, cranial nerve palsies, hepatitis and splenomegaly • The most common features • fever, • lymphadenopathy, • diffuse non irritating rash • condylomatalata
Patchy alopecia of secondary syphilis. Hair loss also occurs commonly from the lateral third of the eyebrows.
Early: Secondary syphilis Malignant syphilis – widespread necrotic papulopustules and ulcers with severe systemic symptoms
Diagnosis of Secondary Syphilis • All serological tests for syphilis are expected to be positive in secondary syphilis • RPR/ VDRL titres in untreated cases are often > 1:8 (VDRL) and > 1: 16 (RPR) • If a specific treponemal test is used for diagnosis and is found to be positive, use the VDRL/ RPR test to determine disease activity, and to monitor response to therapy
Early Latent Syphilis • Diagnosed by a POSITIVE SEROLOGY without symptoms and signs in a person known to be sero-negative in the previous 2 years
LATE SYPHILIS: > 2 years • Late latent: Asx • Benign Tertiary Syphilis (Gumma) • 1 – 45 (average 15) years after infection, • destructive granulomatous lesions on skin, bones • Cardiovascular Syphilis • 15 – 30 yrs • Neurosyphilis: at any stage of syphilis, earlier in HIV patient
Tertiary syphilis (3 – 12 years later) Necrotic nodules or plaques Gummas on lower limb
Late: Benign Tertiary syphilis Gummatous Syphilis • Nodules on skin, bones, • Can also involve the kidney, heart, brain and respiratory
Late: 3. Cardiovascular Syphilis • Aortitis (Proximal aorta) • Aortic incompetence causing Heart failure • Coronary ostialstenosis • Aortic medial necrosis causing aortic aneurysm
Late: 4. Neurosyphilis Involves CNS Meningovascular (MV) or parenchymatous syphilis Sx of MV syphilis: Headache, vertigo and CN palsy Parenchymatous: General paresis of insane
Parenchymatous syphilis • GPI: gradual personality change, ataxia, stroke, opthalmic involvement and tabes dorsalis (lightning pain, sensory impairment and mobility problem) • Rx: Admit for Ix (LP) and IM/IV antibiotic.
Serology interpretation 34 years old female G3P2 at 12 weeks came for booking. Below the serology finding Interpretation?
Serology interpretation 42 years old Malay male, Asx came for VDRL screening as his pregnant partner was treated for syphilis. Below his serology result.
Serology Interpretation 23 years old Male history of painless penis ulcer for 5 days. History of visit to Thai border recently Below the serology result Next step?
Treatment • Early Syphilis - IM Benzathine Penicillin 2.4 mega units single dose or - IM Procaine Penicillin G 600,000 daily x 10/7
Early Syphilis: For patients allergic to penicillin: • T. Doxycycline 100 mg bd x 14/7: (contraindicated in pregnancy) • T. Erythromycin 500 mg qid x 14/7 • T. Erythromycin ES 800 mg qid x 14/7 • IM Ceftriaxone 250 mg daily x 10/7 • T. Azithromycin 2 G single dose • Erythromycin should not be used because of the high risk of failure to cure the foetus. • If erythromycin is used, paediatricians must be alerted and babies have to be treated prophylactically with penicillin and monitored.
Penicillin allergy in Pregnant Women • Should be meticulously interviewed regarding the validity of the history. • Currently, no proven alternative therapies to penicillin, for treating neurosyphilis, congenital syphilis or syphilis in pregnancy. • Therefore, skin testing, with desensitisation, if indicated, should be done for these patients.
MANAGEMENT OF PATIENTS WITH HISTORY OF PENICILLIN ALLERGY • Desensitisationshould be done in a hospital setting because serious IgE-mediated allergic reactions may occur. • A protocol is recommended (refer STI guideline). • Oral penicillin in increasing concentration is administered every 15 minutes. Sensitisation is completed within 4 hours with a cumulative dose of 1.3 million units of penicillin V.
Jarisch-Herxheimer reaction • An acute febrile illness with headache, myalgia, chills and rigors and resolving within 24 hours. • This is common in early syphilis but is usually not important unless • neurological or ophthalmic involvement or • in pregnancy when it may cause fetal distress and premature labour (second half of pregnancy)
Jarisch-Herxheimer reaction • It is uncommon in late syphilis but can potentially be life threatening if there is involvement of strategic sites (coronary ostia, larynx, nervous system). • Prednisolone can reduce the reaction. Recommendation • In early syphilis : Treat with Paracetamol • In Neurosyphilis, Cardiovascular, certain cases of benign tertiary and late latent syphilis: • Treat with Prednisolone 40-60mg daily for 3 days: begin 24 hours before treatment and for 2 days after starting treatment.
ADVICE • Abstain from sex until 1 week after they and their partner(s) have completed treatment. CONTACT TRACING • Examine and investigate all sex partners and treat epidemiologically. • Primary syphilis, notify sexual partners within the past 3/12. • Secondary syphilis with clinical relapse or in early latent syphilis: 2 years • All patients should be offered patient and provider referral as a method of contacting any sexual partner. The method agreed upon with the patient should be clearly documented. • Epidemiological treatment for asymptomatic contacts of early syphilis is recommended.
Incubating/ Epidemiological Rx: Partner • IM B. Penicillin 2.4 mega units single dose or • T. Doxycycline 100 mg bd x 14/7 or • T. Azithromycin 1 G single dose
F/UP for TPHA Positive in Pregnancy • Repeat VDRL/RPR titre • 1/12 after last dose • then monthly until delivered and then • 3/12ly – 6/12ly as non-pregnant women until seronegative or at low titre.
Treatment 2. Late Latent Syphilis • Inj. Benzathine Penicillin 2.4 million i.m once a week for 3/52 i.e. 3 doses Gap between doses: < 14/7. If missed< repeat whole cycle of Rx. • Or IM Procaine penicillin G 600,000 units for 17 days
For patients allergic to penicillin: T. Doxycycline 100 mg oral bd x 28/7 (c/i in pregnancy) or Erythromycin 500mg q.i.d P.O for 28 days Erythromycin ES 800mg q.i.d P.O for 28 days
Follow-up of Late Syphilis Examine and 6 monthly VDRL x 2 years then yearly until seronegative or low titre (1:4 or less)
Congenital Syphilis Rx if sero-positive mother is • Untreated • Rx < 1/12 before delivery • Rx with non penicillin regime • Titre of VDRL not decreased as expected • Treated but insufficient serologic f/up
Syphilis: Rx Failure and Re-Rx • Clinical Sx persist • Initial High titre VDRL failed to decreased fourfold by 1 year • Sustained four fold increase of VDRL titre
Syphilis: Persistent Reactor Titre VDRL persistently > 1:4 despite retreatment with B. Penicillin and trial of treatment with Doxycycline for 28 days when she was not pregnant.
FLOW CHART FOR GENITAL ULCER SYNDROME Patient c/o GENITAL ULCER or SORE Take History and Examine • Investigations • Tzank smear • Gram stain for H. ducreyi • Dark ground microscopy • RPR/TPPA, HIV Ab, anti-HCV, HBsAg • Consider Urine Pregnancy Test ULCER present ?
FLOW CHART FOR GENITAL ULCER SYNDROME (cont’d) ULCER present ? NO • Educate behav change • TCA 2/52 – review result YES Single painless/ multiple painful ulcers Painful grouped vesicles, erosions, ulcers • Treat for Syphilis and Chancroid • Educate for behavior change • Advise sex abstinence for 2 weeks • Provide condom or promote usage • Partner management • Follow-up after 7 days for results • Repeat swabs if positive • Repeat VDRL/RPR, HIV Ab, HBsAg after 3/12 • Genital herpes Mx • Educate for behaviour change • Review after 7 days for results
FLOW CHART FOR GENITAL ULCER SYNDROME (cont’d) ULCER present ? NO • Educate behav change • TCA 2/52 – review result YES Single painless/ multiple painful ulcers Painful grouped vesicles, erosions, ulcers Treat for Syphilis and Chancroid Educate for behavior change Advise sex abstinence for 2 weeks Provide condom or promote usage Partner management Follow-up after 7 days for results Repeat swabs if positive Repeat VDRL/RPR, HIV Ab, HBsAg after 3/12 • Genital herpes Mx • Educate for behaviour change • Review after 7 days for results
Treatment For Genital Ulcer Syndrome FIRST CHOICE IM Benzathine Penicillin 2.4 million units single dose Plus Azithromycin 1.0 gm single oral dose Treatment For Syphilis and Chancroid SECOND CHOICE IM BenzathinePenicilline 2.4 million units single dose Plus IM Ceftriaxone 250 mg single dose If patient develops allergic reaction to 1st dose of IM B. Penicillin, do not give the 2nd dose. If allergic to B. Pen: Doxycline 100 mg bd x 14 days or EES 800 mg qid x 14/7 Doxycycline: should not be used during pregnancy, lactation or children. Babies of mothers who are treated with Erythromycin must be treated for syphilis.
REMINDER • For all pregnant lady and partner with TPHA positive, don’t forget to screen for other STIs i.e: • HIV Ab, HCV, HBsAg • GC smear • TV wet smear