Download
1 / 48
480 likes | 505 Views
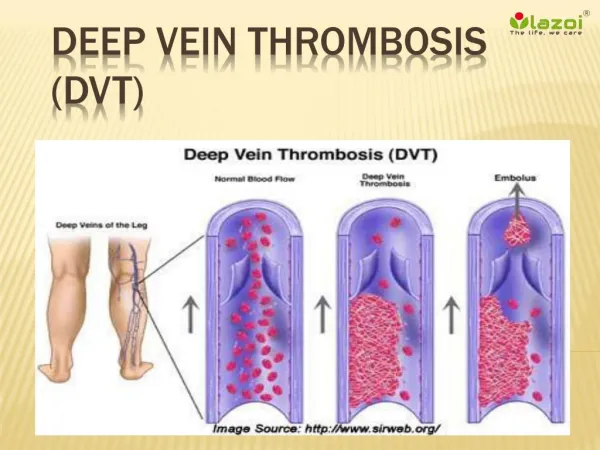
Prevention and Prophylaxis of Deep Vein Thrombosis. Kofi Ametih St Benito Menni Hospital. What makes VTE so dangerous. The illness is often "silent" and can mimic other common conditions such as heart attack, pneumonia, and anxiety.

E N D
Prevention and Prophylaxisof Deep Vein Thrombosis Kofi Ametih St Benito Menni Hospital
What makes VTE so dangerous • The illness is often "silent" and can mimic other common conditions such as heart attack, pneumonia, and anxiety. • Many healthcare providers are under the false impression that this life-threatening illness is not a problem in their hospital or among their patients.
How serious is the problem? A very serious problem • 80% of PE occur without signs • 2/3 of deaths occur within 30 minutes A common problem • Estimated 1:100 hospitalized patients dies of PE Can be prevented • ½ of all PE, 2/3 of all DVT preventable in a review of 16,000 patients Should be prevented • More extensive use of prophylaxis
Risk factors • Lifestyle: Common lifestyle risk factors for VTE are same for cardiovascular disease: obesity, inactivity, and cigarette smoking. • Trauma • Accidental trauma • Surgical / iatrogenic trauma -orthopaedic surgery (hips and knees) -major surgery lasting > 30 minutes
Additional risk factors • Age (risk rises steadily from age 40) • Malignancy • History of previous DVT or PE • Immobilization (bed rest, paralysis of legs, plaster casts) • Pregnancy and puerperium • Oral contraceptive use • Extensive dissection at surgery
Clinical disorders predisposing to venous thrombosis • Varicose veins • Cardiac problems (e.g. cardiac failure and myocardial infarction • Stroke • Nephrotic syndrome • Thrombocytosis • Primary proliferative polycythaemia • Systemic lupus erythematosus • Infection
The special risk in surgical patients • Unwell and may have been immobile or inactive. • Bed rest, immobility post op, traction, plaster casts. • Direct vascular damage, kinking or twisting of major veins, pressure on large veins. • Tissue damage from dissection ↑se activated coagulation factor levels. The more extensive the damage, the more likely activation of coagulation. • Surgery lasting > 30 to 45 minutes considered at risk. • Spinal and epidural anaesthetics seem to be less thrombogenic than GA
Low Risk General medical patient Uncomplicated minor surgery in patients < 40 yrs with no clinical risk factors Moderate Risk Major surgery in patients older than 40 yrs with no other clinical risk factors Risk stratification
High risk Major surgery in patients > 40 years, who have additional risk factors or MI Very high risk Major surgery in patients > 40 years plus Previous VTE or malignant disease or orthopaedic surgery or hip fracture or stroke or spinal cord injury Risk stratification ctd
Ideal primary prophylactic agent • Effective • Free from clinically important side effects • Well accepted by patients, nurses and medical staff • It should be easy to administer • Relatively inexpensive • Require minimal monitoring
Methods of primary prevention • Mechanical methods- increase venous blood flow in the leg veins. • Pharmacological agents - suppress activation of blood coagulation
Mechanical methods Mechanism of Prevention • Stimulate calf muscles and put pressure on the calf and leg veins, thus discouraging stasis and venous pooling of blood in the lower extremities.
I. Early mobilization • Admitting elective surgery patients close to day of surgery (reduced mobility in hospital even when well). Complete all investigations as an outpatient • Early mobilization of patients as soon as possible after surgery • Physiotherapy • Encouraging mobilization of medical patients who are well enough to do so
II. Graded compression stockings • Should be fitted individually to ensure that pressure is correctly graded (highest at the ankle and decreases in a proximal direction). • Should be considered in all at-risk surgical and medical patients • Routine for all in-patients in some hospitals
Pressure gradient on a compression stocking Popliteal 8mmHg Lower thigh 10mmHg Calf 14mmHg Ankle 18mmHg Upper thigh 8mmHg
Sizing to achieve the gradient
Class 1 G.C.Stocking (Pressure at ankle 20 – 30 mmHg)Used for greater support e.g. previous DVT, minor swelling or ongoing discomfort) May also be used to prevent DVT in flights. Class 2 G.C.Stocking (Pressure at ankle 30 – 40 mmHg)Used when more support is required. Recent DVT, significant swelling of the leg Class 3 G.C.Stocking (Pressure at ankle 40+ mmHg)Used for maximal support, e.g. veins are damaged and there is long term swelling of the legs Class 1 and 2 stockings may be purchased at a pharmacy, Class 3 stockings need to be specially made for patients. Indication is also important
III. Intermittent pneumatic leg compression • Enhances blood flow in the deep veins of the legs. • Useful in patients at high risk of bleeding from anticoagulants, e.g. neurosurgery, major knee surgery and prostatic surgery. • May be as effective as low-dose heparin
Pharmacological agents • Mechanisms of action • These agents prevent, to differing degrees, thrombus formation by • Interfering with blood coagulation (heparin, warfarin) • Enhancing blood flow and fibrin stability (dextran).
Heparin prophylaxisa) Low dose heparin • 5000 IU every 8 or 12 hours in all patients • Surgical pts, 1st dose may be given 2 hours pre-op • Fear of bleeding intra-op, 1st dose may be delayed until immediately post-op. • Continued for about 7 days in surgical pts or until patient becomes fully ambulatory. • Does not require laboratory monitoring • Simple, fairly convenient to administer. • A method of choice for moderate to high-risk surgical and medical patients • Can ↓ the risk of VTE by 50 to 70%.
Effectiveness of low dose heparin • 22% to 9% in general surgery, i.e., a 59% risk reduction • 48% to 24% in orthopaedic surgery, i.e., a 50% risk reduction • 41% to 14% percent in urological surgery, i.e., a 68% risk reduction.
Cautions -low dose heparin • Potential to cause minor bleeding • Contraindicated in patients with known heparin sensitivity, defect in haemostasis, severe hypertension, and when there has been a hemorrhagic accident. • Less effective than adjusted-dose heparin, oral anticoagulants or LMWH.
b) Adjusted dose heparin • 8-hrly sc heparin (begun 2 days pre-op) • Starting dose is 3,500 U, subsequent dose-adjusted steps of 500 to l000 U 8 hourly to achieve an APTT in the upper normal range 6 hours after injection, i.e. 25 – 35 secs • Obviously more complicated • Requires more monitoring than low-dose heparin • More effective than low dose heparin in very-high-risk patients.
c) Low molecular weight heparins • Most effective form of prophylaxis in hip surgery, knee surgery, general surgery and following major trauma. • Longer half-life than standard heparin, highly effective and safe, once daily dose • Superior to dextran. • Enoxaparin, dalteparin and ardeparin
LMWHs - Dosing regimens • High-risk patients, enoxaparin is given in a dose of 40 mg once a day, 1st dose given 2 hrs pre-op, repeated once daily until the risk of thrombosis is thought to have diminished • Very-high-risk, enoxaparin given at a dose of 30 mg twice daily,1st dose 12 hours post-op, doses repeated twice daily until risk of thrombosis is considered to have passed. • Currently much interest in continuing to administer LMWHs for a longer period after surgery to protect against the longer-term threat of thrombosis.
LMWHs- effectiveness • Studies in stroke patients suggest from 60 to 80% relative reduction in thrombosis risk by administering LMWHs prophylactically • Similar reduction in bedridden patients • Many experts now believe that the efficacy and ease of use of these compounds make them the prophylaxis of choice in most very-high-risk patients.
e) Dextran • 1. Differing molecular weights, dextran-40 and dextran-70, • Plasma vol expander, ↓ blood viscosity, ↑ blood flow and ↓ venous stasis. • Infused from time of surgery over of 4 to 6 hours, then daily for 2 to 5 days post-op. • 2. 500ml D-40 daily over 1st 3 to 5 days post-op, then additional doses every 3rd day till patient ambulates. • Less effective than warfarin or LMWH in preventing DVT. • Associated with allergic reactions or bleeding in some patients, potential for volume overload. • For these reasons dextran has not been widely adopted
d) Warfarin • Administered to obtain INR of 2.0 to 3.0 • Effective in preventing post-op thrombosis in all risk categories. • Can be started • Pre-op, • At time of surgery • Immediately after surgery
Examples of Methodology • 1.3 mg 10 to 14 days pre-op with the aim of adjusting the INR to 1.3 to 1.5 at the time of surgery • Gradually ↑se dose to an INR of 2.0 to 2.5 at 3 to 4 days post-op. • Relatively safe approach but impractical since it requires many days of careful monitoring. • 2. 5 mg on the evening of the operation or the 1st post-op day, aiming for INR of 2.0 to 3.0 on the 4th or 5th post-op day. • More practical approach, effective and relatively safe but still requires careful laboratory monitoring.
Summary of efficacy of various prophylactic approaches with venography as the endpoint
Using the current methods of prophylaxis • Exactly when and for how long should prophylaxis for VTE be given. • Should pharmacological prophylaxis begin pre- or postoperatively? • How long should a course of prophylaxis last? • Are there differences in the type, dose and duration of prophylaxis to be used in different risk groups?
Choice of prophylaxis in different patient groups • Decision to use prophylaxis mostly based on the presence of one or more of risk factors known to predispose pts to post-op or medical VTE • Attempts to refine this process by adding laboratory tests to the clinical risk factors and deriving formulae in which risks are weighed to yield a predictive index for a given patient. • Most of these indices have not proved helpful, and, consequently, the best approach is still for doctors to rely on their knowledge of risk factors and to weigh the benefits of prophylaxis for each patient.
Low-risk patients • General medical patients, surgical patients < 40 years who undergo minor operations (G.A. lasting < 30 minutes) appear to be at a low risk for DVT. • Early ambulation should provide adequate protection in this group of low-risk patients.
Combined approach for high/very high risk patients • Stockings alone not sufficient • Combining vascular compression stockings with low-dose heparin is an effective strategy for patients at high or very high risk of VTE. • 10- to 18-mm Hg graduated compression stockings or pneumatic compression boots plus heparin 5000 U every 8 hours or LMWH in patients undergoing high-risk surgeries.
Added risk, prophylaxis: pre- or postoperative? • Concern from fear of bleeding from pre-op prophylaxis • Studies show safety of starting pre-op • Many surgeons do not wish to begin prophylaxis, even with LMWHs, pre-op. • Prefer instead to begin with 1st dose of heparin or LMWH 12 hrs post-op, especially when spinal anaesthesia was used.
For how long should prophylaxis continue? • No one actually knows how long the danger of VTE persists after surgery • Study of patients after their discharge from the hospital following major surgery confirmed that the risks of developing VTE disease can extend beyond the patient's stay in the hospital. • Once patients return home, they may be even less mobile than when they were in the hospital • 57 patients studied, 13 developed DVT during the 6 weeks after surgery
How long? - ctd • Many patients receive heparin or LMWH for about one week after surgery and are then switched to oral anticoagulants for several weeks to provide some continuing protection at home. • In Ghana, UFH of LMWH followed by warfarin for about 6 weeks at home seems a workable and economically more feasible option for high risk patients
General or selective prophylaxis ? • Swedish study: compared cost effectiveness of three alternatives in patients 40 years and older who underwent • general surgery (low risk) • surgery for cholelithiasis (moderate risk) • elective hip surgery (high risk) • • no prophylaxis • • general prophylaxis with low-dose heparin • • selective therapy following screening with fibrinogen-uptake alone or with venography.
General or selective prophylaxis • From this study, it emerged that general prophylaxis was the best option in terms of reducing the frequency of venous thrombosis - a reduction of 70%. • General prophylaxis was also the best approach to reducing patient mortality after surgery.
Recommendations • All patients suspected of being at risk of venous thrombosis should be encouraged to keep mobile. • Indeed, in all patients, early ambulation and graduated compression stockings should be considered automatically on admission. • Patients in high-risk groups should receive, in addition, pharmacological prophylaxis.
In-flight prophylaxis • Economy class syndrome, travellers thrombosis • Unknown factors additional to immobility may lead to flight-related DVT • Those with predisposing risk factors are at greatest risk of flight-related DVT and should consider preventative measures. • The highest risk groups include the elderly, pregnant women, those suffering serious medical conditions such as cancer and those with recent orthopaedic surgery (legs or knees).
Incidence, mechanism • Low occurrence and often asymptomatic. • Chance of massive PE and death is only about 1 in 1,000,000 travellers. • Limited evidence available • Estimated incidence of DVT • symptomatic 0% to 0.28% • asymptomatic 0% to 10.34%. • Mechanism-Hypobaric hypoxia: can occur due to • decreased pressure in the aircraft cabin • diminished supply of airborne oxygen • induce coagulation.
The WRIGHT Project (World Health Organisation Research Into Global Hazards of Travel) • Report that risk of VTE approximately doubles after a long haul flight of>4 hours • Also occurs in other forms of travel where travellers are exposed to prolonged seated immobility.
Prevention of Economy Class Syndrome • Adequate hydration (drinking, abstaining from alcoholic beverages and caffeine ), moving around and calf muscle exercises • Any traveller with significant risk factors should seek medical advice and consider prophylaxis. • Aspirin is not recommended • LMWH may be considered for high-risk individuals embarking on a long-haul flight. • Elastic compression stockings reduce asymptomatic DVT and leg oedema associated with air travel in all risk groups.
Summary • Regimens recommended for prevention of DVT and PE include mechanical and pharmacological methods. • Combination mechanical plus pharmacological most effective in high risk patients • Aspirin has not been shown to be beneficial. • None of these preventive measures is ideal but most are relatively simple to use; complications are generally minor and the need for laboratory monitoring is minimal.
Thank you