Download
1 / 22
250 likes | 282 Views
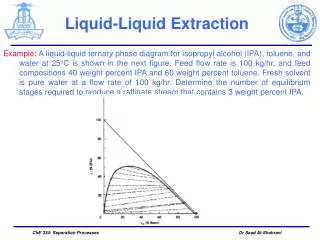
Renovascular hypertension Dr Saad Al Shohaib KAUH. Incidence. Renovascular disease is an important and treatable cause of hypertension and renal impairment It accounts for less than 1% of mild and moderate hypertension but may be seen in 10 to 40% of hypertensive crises

E N D
Incidence • Renovascular disease is an important and treatable cause of hypertension and renal impairment • It accounts for less than 1% of mild and moderate hypertension but may be seen in 10 to 40% of hypertensive crises • Renal disease is the comments cause of secondary hypertension
Target population for screening • Acute rise in serum creatinine shortly after ACE inhibitor therapy or unexplained rapid deterioration in renal function with minimal proteinuria • Moderate to sever hypertension in a patient with diffuse atherosclerosis • Hypertension in a patient with a symmetric renal size or hypokalemia • Moderate to severe hypertension in patients with recurrent episodes of acute (flash) pulmonary edema or otherwise unexplained congestive heart failure
Screening tests • Intravenous pyelogram – There are two major findings on intravenous pyelography that suggest the presence of unilateral ischemia: a decrease in renal size; and delayed caliceal appearance time when compared to the contralateral kidney
Screening • Plasma renin activity – The baseline plasma renin activity is elevated in only 50 to 80 percent of patients with renovascular hypertension • . The predictive value can be increased by measuring the rise in the plasma renin activity one hour after the administration of 25 to 50 mg of captopril
screening • Renogram following ACE inhibitor • the predictive value of radioisotope scanning can be increased by enhancement with captopril.
Screening • Duplex Doppler ultrasonography has the advantage of providing both anatomic and functional assessment of the renal arteries • Time consuming • Operator dependent and difficult • It can be done after captopril
Recommendations • In high risk patients may use subs traction angiogram as an initial test • MR angiography is a non invasive alternative test particularly if combined with doppler
In one study 38 patients with hypertension were screened using MRA and subs traction angiogram • One patient was excluded 14 patients had renal artery steno sis • 12 patients had more than 50% stenosis Postma CT Joosten FB etal AM J Hyper sept 1997
All these stenos is were recognized by MRA • There were one false positive case by MRA • MRA has 100% sensitivity and 96% specifity Postma CT; Joosten FB; Rosenbusch G; Thien T SO - Am J Hypertens 1997 Sep;10(9 Pt 1):957-63
Conclusion • MRA has a great accuracy in detecting clinically significant main renal artery stenos is
Significant stenosis • Hem dynamically significant stenos only should be corrected • Good response to ACE inhibitors suggest the presence of significant stenos • increased Renal vein renin may suggest a significant stenosis but this is not widely used • Other tests used to screen for renovascular hypertension would help to determine significance
CRF AND ISCHAEMIA • Ischemia might be responsible for decreased renal function in a significant number of patients with renal failure in older patients • Correction of ischemia would improve renal function
Renal insufficiency • Unexplained progressive renal failure • Benign urine sediment with sever renal impairment • Unilateral very small kidney with renal impairment • Testing should be done with progressive renal impairment uncontrolled pressure and recurrent pulmonary edema • Contrast may induce further renal damage
Ischemia and CRF • Presence of diffuse atherosclerosis make Reno vascular disease more likely • There is usually minimal proteinuria • Uncontrolled hypertension • Flash pulmonary edema • Progressive renal failure with benign urine sediment
Renovascular disease • The earlier the intervention the better the prognosis • Contrast may cause further renal damage • Reversibility is more likely in patients with rapid deterioration of renal function
Conclusion • Renovascular hypertension should be suspected in hypertensive crisis uncontrolled hypertension patients with hypokalemia and high BP • Presence of unequal kidney size or flash pulmonary edema make the diagnosis more likely
Conclusion • The homodynamic effect of ِِACE inhibitors help in the diagnosis reversibility of renal function as well as the significance of the stenosis • Uncontrolled hypertension in a patient with diffuse atherosclerosis particularly if associated with renal impairment is highly suggestive of renovascular hypertension
Conclusion • MRA with Doppler ultrasound are good screening tests • Revascularization should be done in hem dynamically significant stenosis • Correction of significant bilateral stenosis may improve renal failure and help to avoid dialysis in selected cases