Download
1 / 68
680 likes | 688 Views
Operating Room Metrics Applied to Hospital Service Contracts ASA Conference on Practice Management Pre-Conference AACD Friday January 29, 2010 10:15-11:30 Joe Laden Business Manager Anesthesia Associates of Louisville, PSC Since 1981

E N D
Operating Room Metrics Applied to Hospital Service Contracts ASA Conference on Practice Management Pre-Conference AACD Friday January 29, 2010 10:15-11:30 Joe Laden Business Manager Anesthesia Associates of Louisville, PSC Since 1981 20 MD’s & 30 CRNA’s Serving Norton Hospitals for 30+ Years joeladen@aalouisville.com
Objectives • To define and illustrate several operating room metrics that can be applied to anesthesia service contracts.To demonstrate how operating room metrics can be used in anesthesia service contracts to calculate hospital financial support.
Types of Operating Room Metrics Used in Anesthesia Service Contracts Specify the number of anesthetizing locations the contracting anesthesiology group will cover including hours and days of coverage. As elements of practice performance standards. In the calculation of hospital financial support (stipends)
1. OR Metrics Specifying Operating Room Coverage • Number of ORs covered • Hours of Operation of ORs
The Number of Operation Rooms to Be Staffed By the Anesthesia Group is a Simple Metric but . . . If not specified properly in the contract, this can be a problem for the group
ANESTHESIA SERVICES AGREEMENT • “Anesthesia locations” shall be defined as all those services in Hospital where anesthesia services are required, including, but not limited to, operating rooms, cardiac catheterization labs, lithotripsy, ECT therapy, and certain imaging procedure rooms. Anesthesia Services from Group shall be available according to the following schedule: • Monday through Friday: fully staffed and scheduled coverage is required for: • Six(6) anesthesia locations from 7:00 a.m. to 3:00 p.m. • Two (4) anesthesia locations from 3:00 p.m. to 5:00 p.m. • Saturday: fully-staffed and scheduled coverage shall be available for two (2) anesthesia locations from 7:30 a.m. through 3:00 p.m. • Sundays and weekday holidays: coverage is required for cases performed when the operating surgeon determines that the procedure is urgently necessary for the benefit of the patient. • Emergency on-call coverage shall be provided for one (1) anesthesia locations twenty-four (24) hours per day, Monday through Sunday. • Group shall provide pre-admission consultation services for patients scheduled to receive anesthesia, in collaboration with the Hospital Pre-Admission Testing service.
“Anesthesia locations” shall be defined as all those services in Hospital where anesthesia services are required, including, but not limited to, operating rooms, cardiac catheterization labs, lithotripsy, ECT therapy, endoscopy and certain imaging procedure rooms. Anesthesia Services from Group shall be available according to the following schedule: • Monday through Friday: fully staffed and scheduled coverage is required for: • Six (6) anesthesia locations from 7:00 a.m. to 3:00 p.m. • Two (2) anesthesia locations from 3:00 p.m. to 5:00 p.m.
Saturday: fully-staffed and scheduled coverage shall be available for two (2) anesthesia locations from 7:30 a.m. through 3:00 p.m. Sundays and weekday holidays: coverage is required for cases performed when the operating surgeon determines that the procedure is urgently necessary for the benefit of the patient. Emergency on-call coverage shall be provided for one (1) anesthesia locations twenty-four (24) hours per day, Monday through Sunday. Group shall provide pre-admission consultation services for patients scheduled to receive anesthesia, in collaboration with the Hospital Pre-Admission Testing service.
Operating Room Coverage Specified in Hospital Contract • Number of ORs covered (staffed) • Days of Week ORs are covered • Beginning and Ending Hours of Coverage • Type of Coverage (sub-specialty)
Example: Group agrees to cover 12 ORs but . . . Hospital expects coverage of endo suites “when needed” even when all 12 ORs are in operation
Alternate Anesthetizing Locations • Cath Lab • MRI • Radiology • Endoscopy Suite • Lithotripsy
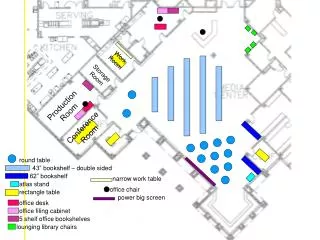
Handling the Number of ORs Potential Problem • Contract should specify in some form that group will be responsible for coverage of no more than N simultaneous anesthetics. • Coverage in out of operating room locations should be scheduled from existing operating rooms. • Example: • OR 2 • 7:30 D&C • 8:30 Anesthesia to MRI • 11:00 Hysterectomy
“Anesthesia locations” shall be defined as all those services in Hospital where anesthesia services are required, including, but not limited to, operating rooms, cardiac catheterization labs, lithotripsy, ECT therapy, endoscopy and certain imaging procedure rooms
The time of an anesthetic should include: • Time to interview the patient and place lines and post operative pain blocks. • Time to bring patient to recovery room • For non-operating room locations, travel time to location should be included.
Definition of Beginning of Coverage Does 7:00 a.m. mean “room ready”, “patient in OR”, “anesthesiologist reporting time” or “cut time”? Example: If contract beginning coverage time is “cut time” at 7:00 then anesthesia personnel need to be in the hospital – and paid – from 6:15-6:30 especially for cases with lines and regional blocks.
Ending Time of Anesthesia Coverage Usually means the time of day after which anesthesia personnel are no longer needed on a continuous basis in the operating rooms referenced.
What Happens if Case Time Extends Past Contracted Coverage End Time? • Anesthesia group wants to accommodate surgeons • Running ORs late can end schedule earlier • Late ORs can be an opportunity for extra billing • But • Will need to pay overtime or fund late shifts • Habitual lateness wears on staff • Not funded by hospital if not in contract • Non prime hours are paid at same rate by third party payers
Example: Group receives an inadequate $259 per hour from third party payers. Actual cost to deliver services is 26% higher or $326. Personnel costs are 50% higher after hours Reimbursement from hospital will be: $326 X 1.5 = $489 less $259 collected from payers resulting in a net of $230 per hour.
What Happens if Case Time Extends Past Contracted Coverage End Time? • Contract can specify monetary penalty for coverage overruns • e.g.: Hourly rate for case hours beyond hours specified in contract, billed to hospital monthly (less collections for this time period) • Contract renegotiated if hours beyond coverage specified in contract exceed a certain number or percentage of total hours to be covered
Virtual Operating Room Problem • Contract specifies coverage for 12 ORs and hospital is licensed for 12 ORs, but actually has 14 ORs • Hospital wants to use extra ORs for “flipping rooms” • This should be addressed in contract as coverage for 14 ORs for certain days and hours • Flip rooms usually have lower utilization and need additional financial support from the hospital
Review of Potential Contractual Problem Areas • Number of simultaneous anesthetics • Beginning Coverage Time • Ending Coverage Time • Out of Operating Room Coverage • Virtual operating rooms
Bottom Line: When initiating or renegotiating a hospital service contract, precisely define Number of ORs covered, Operating Times and any financial remuneration from the hospital for coverage overruns. Suggestion: Review your current contract and actual hours of coverage provided by group when you return from this meeting. You are probably providing uncompensated services in excess of that specified in your contract.
2. Practice Performance Standards Related to Operating Room Metrics
Typical Practice Performance Standards/Measures in Anesthesia Service Contracts • Adherence to hospital rules • Scores in patient surveys • Scores on surgeon surveys • Physician behavior • Attendance at hospital meetings • Compliance with Joint Commission measures • Adherence to documentation standards • Use of low-cost drugs and disposable supplies • PQRI participation
STANDARDS OF PERFORMANCE REPORT FOR ANESTHESIA SERVICES Scorecard
Practice Performance Standards Related to OR Metrics • Percentage of cases cancelled by anesthesia • Percentage of cases delayed by anesthesia
Practice Performance Standards Related to OR Metrics • May be part of overall “scoring” system that could cause review or cancellation of the anesthesia service contract. • These measures should be clearly defined in contract and that the group has a method to review and correct erroneous reporting by hospital. • Performance standards scores could be tied in to financial support.
3. Calculating Hospital Financial Support Based on Operating Room Metrics
Two OR Metrics That Can Be Specified in a Hospital Service Contracts • Operating room utilization percentage • Percentage of case time outside prime hours (e.g. outside7:00 a.m. – 3:00 p.m. weekdays)
Types of Hospital Financial Support Fixed amount OB coverage In-house Call Stipend Trauma Stipend Medical Directorship Pre-admisson Testing Clinic Negotiated “Gap” amount CRNA Support
Types of Hospital Financial Support Variable Amount Revenue Guarantee Low Utilization Supplement Excess/Late Hours Supplement Payer Mix Support Coverage Overrun Penalty Locum Coverage Payments
The Problem of the “GAP” Personnel Cost to Provide Contracted OR Coverage Greater Than Patient Revenue Less Billing Costs Resulting in a Need for Hospital Financial Support to close the gap.
Personnel Cost Is Determined by: • Number of personnel to provide OR coverage specified in anesthesia service contract by number of operating rooms and hours of operation. • Prevailing area MD and CRNA salary and benefit requirements. • Both of these factors are mostly out of the control of the anesthesiology group.
Patient Revenue is Determined by: • Payer Mix • Units or Hours Billed Per Operating Room • Both of these factors are out of the control of the anesthesiology group.
Payer mix by hourly rate will be easier for hospital administrators to understand than ASA RV units
Example: Total Practice Budget to Cover 20 ORs Personnel Cost + Billing cost + Other Corporate Overhead = $9,000,000 Cost per OR per day: $1,800 = $9,000,000 / 250 days / 20 ORs
Example: 20 Operating Rooms 5.5 Average Hours of Anesthesia Time Billed Per OR Patient Revenue = $259/hour of Anesthesia Time Billed Result: 5.5 x $259 = $1,425 per OR per day. Personnel Cost per day = $1,800 Gap = $375 per OR per Day.
Total Gap Calculaton $375 / OR per day x 20 ORs x 250 days = $1,875,000 Total Per Year
The OR Metric that Controls the Magnitude of the GAP is Operating Room Utilization Higher OR Utilization Results in More Hours of Anesthesia Billed Per OR and vice versa Increasing OR Utilization Will Increase Patient Revenue Without Increasing Personnel Needed to Staff the OR
Defining Operating Room Utilization OR utilization measurement can vary depending on definitions of case time an whether turnover time is used. Use hospital’s definition (e.g. AACD Raw Utilization) From your billing system, use anesthesia hours billed during prime time. Main concern is the difference between target utilization and actual utilization.
Two Utilization Problems Can Occur • Hospital/Surgeons Underutilize Contracted Prime Hours • Hospital/Surgeons Overutilize non-Prime Hours
Example: Prime OR hours are 7:00-3:00 (8 hours) We use anesthesia hours billed without turnover time. (slightly > raw utilization) Assume 5 of 5.5 total hours are in prime time Utilization rate is 5/8 = 62.5% Coupled with poor payer mix ($259/hr.) results in considerable gap.
How can the OR utilization rate be increased to reduce the “gap” in this example? • Move Late Cases Into Prime Time (only have .5 hrs.) • Increase Surgical Volume in Existing Operating Rooms • (would need to increase volume 26%) • Reduce Number of ORs, Increasing Volume in Remaining ORs
How can the OR utilization rate be increased to reduce the “gap” in this example? • At $259/hr. it would take 6.95 hours of anesthesia time per OR to generate $1,800 in patient revenue / OR / day (divide $1,800 by $259) • .5 hours occur after prime time, so 6.45 hours will be in prime time • Utilization needs to be 6.45 / 8 = 80.6% (w/o turnover)
Conclusion: 62.5% OR utilization Causes $1,875,000 Gap 80.6% OR utilization brings gap to zero Each percentage increase in utilization reduces gap by $103,591. ($1,875,000 / (80.6% -62.5%))
How Can OR Utilization be Implemented in Hospital Service Contract? • Measure OR utilization on a monthly basis • Hospital pays group $1,875,000 / 12 = $156,250 per month if utilization stays at $62.5%. • This is amount is adjusted upward or downward by $103,591 / 12 = $ 8,633 per month for each percentage change in the OR utilization percentage.