Download
1 / 31
330 likes | 657 Views
Advances in the Treatment of Alcoholic Liver Disease. Dr Allister J Grant Consultant Hepatologist Leicester Liver Unit University Hospitals Leicester NHS Trust. Background National and local perspective Alcoholic Hepatitis Presentation Pathophysiology Prognosis Management

E N D
Advances in the Treatment of Alcoholic Liver Disease Dr Allister J Grant Consultant Hepatologist Leicester Liver Unit University Hospitals Leicester NHS Trust
Background • National and local perspective • Alcoholic Hepatitis • Presentation • Pathophysiology • Prognosis • Management • Corticosteroids and pentoxifylline
The Burden of Alcohol 9 million adults in the UK who are drinking over the recommended daily limits people aged 16-24 are the heaviest drinkers The Royal Liverpool University Hospital, 12% of A&E attendances were shown to be directly related to alcohol In inner city A&E departments approximately 75% of patients attending after midnight are drunk 20% of patients admitted to hospital for illnesses unrelated to alcohol, are drinking at hazardous levels
Alcohol Related Deaths E&W 1991-2004 http://www.statistics.gov.uk/cci/nugget.asp?id=1091
UHL Med/A&E Directorate Alcoholic Hepatitis Alcoholic Liver Disease Alcohol Intoxication Alcohol Withdrawal Alcohol Withdrawal Fits Cirrhosis due to alcohol DTs June 2006- July 2007 942 admissions 4544 bed days 12.5 beds permanently occupied
alcohol induced chronic pancreatitis alcoholic liver disease alcoholic gastritis alcohol abuse counselling & surveillance alcohol rehabilitation alcohol abuse without diagnosis of alcoholism history of alcohol abuse oesophageal varices in alcoholic liver disease and others……… UHL Alcohol Admissions 2004-8
UHL Alcohol Admissions 2004-8 Monthly admission rate
Spectrum of Alcoholic Liver Disease • The most common manifestations of alcoholic liver disease are: • Alcoholic steato-hepatitis • Acute alcoholic hepatitis • Cirrhosis due to alcohol
Alcoholic Hepatitis • Most florid manifestation of ALD • Cholestatic liver disease associated with the long term heavy use of alcohol • Often a precursor to the development of cirrhosis • More severe forms are associated with a high mortality • 1yr mortality after initial hospitalisation is 40% • Best treatment • Stop drinking • Resolution occurs within weeks-months +/- cirrhosis
Symptoms Fever Hepatomegaly Jaundice Coagulopathy Features of hepatic decompensation However, milder forms of alcoholic hepatitis often do not cause any symptoms
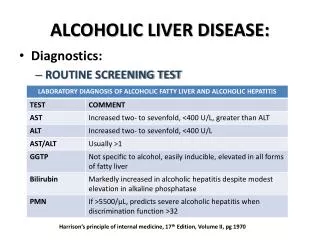
Investigation • Biochemistry • AST/ALT ratio >1.5 • ALT usually <100 IU/ml • Raised GT (variable) • Raised ALP (variable) • Low Albumin (advanced disease) • Bilirubin (≥80 mol/l) • Haematology • Prolonged INR (advanced disease) • Macrocytosis / anaemia • Leukocytosis • Thrombocytopenia (advanced disease)
Investigations 2 • Other • Hyperuricaemia • Hypertriglyceridaemia • Raised IgA • Hyperglycaemia Perform a liver screen Liver Biopsy
Pathology of Alcoholic Hepatitis Mallorys Hyaline Centrilobular necrosis Fatty change Hepatocyte ballooning PMN infiltrate Pericellular fibrosis
Altered membrane proteins Neoantigens formation Impaired cytoskeletal transport Stimulation of HSC Immunological injury Damage to cell membranes Alcoholic Hepatitis Mechanisms of liver injury Free radicals Oxidative injury Heat Gut Permeability Endotoxaemia Kupfer cell activation Gultathione depletion ROS & Free radicals TNFα Alcohol dehydrogenase (ADH) Peroxisomal Catalase Genetics Polymorphisms Male vs Female Race Damage Acetaldehyde Ethanol Miscrosomal ethanol-oxidising system (CYP 2E1) Acetaldehyde dehydrogenase Downregulated in chronic alcohol use TNFα IL-1, IL-8 Acetate
Prognosis Maddrey WC Gastro 1978 Mathurin P J Hepatol 2002 Scoring Systems • DF = (4.66PT)+serum bilirubin (mg/dl) • mDF = 4.6 (PTpatient-PTcontrol)+ serum bilirubin (mmol/l)/17.1 • mDF≥32 68% 28 day survival • mDF<32 93% 28 day survival • MELD = 3.86loge(bilirubin (mg/dl))+1.26 loge(INR)+ 9.66loge(creatinine (mg/dl))
241 patients with alcoholic hepatitis were studied on day 1, 6-9 and variables that predicted outcome at days 28 and 84 were sought. These variables were included in the Glasgow alcoholic hepatitis score (GAHS) and validated against a further 195 patients. 28 days 84 days Bilirubin Albumin Urea WCC PT Encephalopathy Bilirubin Albumin Urea WCC PT Age AST/ALT ratio Factors independently associated with mortality at- Analysis of factors predictive of mortality in alcoholic hepatitis and derivation and validation of the Glasgow alcoholic hepatitis score. E H Forrest, C D J Evans, S Stewart, M Phillips, Y H Oo, N C McAvoy, N C Fisher, S Singhal,A Brind, G Haydon, J O’Grady, C P Day, P C Hayes, L S Murray, A J Morris Gut 2005;54:1174–1179.
Glasgow Alcoholic Hepatitis Score Score 1 2 3 Patients score from 5-12 points. Score >8 was used to define the high risk population and maximised sensitivity and specificity. Age <50 ≥ 50 WCC(109/l) <15 ≥15 Urea (mmol/l) <5 ≥5 PT ratio <1.5 1.5-2.0 >2.0 Bili (mol/l) <125 125-250 >250
GAHS Validation Cohort 28 day outcome (%) Sensitivity Specificity Accuracy Day 1 GAHS </≥9 81 61 67 mDF </≥32 96 27 48 Day 7 GAHS</≥9 93 68 75 mDF </≥32 90 45 56 195 patients with Alcoholic Hepatitis GAHS score calculated on days 1,7 and correlated with outcome
Survival from Alcoholic Hepatitis Derivation and validation datasets combined – 436 patients 28 day survival (%) 84 day survival(%) Day 1 GAHS <9 87 79 GAHS ≥9 46 40 Day 7 GAHS<9 9386 GAHS ≥9 4737
Why is a prognostic score important? Patients with mild alcoholic hepatitis will improve spontaneously upon cessation of alcohol Patients with severe alcoholic hepatitis should be monitored in level 2 care or above A significant percentage of patients will deteriorate some time after initial presentation Patients with severe alcoholic hepatitis benefit from the initiation of specific therapies
Management of Alcoholic Hepatitis • General • Stop drinking alcohol • Treat alcohol withdrawal • Thiamine/Vit B • Pabrinex • Treat malnutrition (po/ng) • Vit K if INR prolonged • Treat hepatic decompensation
Therapy The following therapeutic agents have been used in alcoholic hepatitis • Evidence • to support the use of: • Corticosteroids • Pentoxifylline • Nutritional support • Insufficient evidence to support the use of: • Anabolic steroids • Infliximab • Etanercept • Malotilate • No evidence • to support the use of: • PTU • Insulin & glucose • Colchicine • Antioxidants
Nutritional support • Multifactorial- • poor intake/malabsorption/catabolism • No published guidance (Vit B/ Vit K/ Zinc) • Mortality is significantly associated with protein-energy malnutrition • Mild vs. severe nutritional deficiency • 30 day mortality= 2% vs. 52% Meadenhall CL Am.J.Clin.Nut 1986
Nutritional support • PEM is virtually universal- refeeding! • Evaluated in several clinical trials • Results in a more rapid improvement in liver disease • Does not improve survival Henkel AS, Nat.Clin.Pract.Gastroenteol.Hepatol 2006 Stickel F, APT 2003 • 1.2-1.5g protein and 35-40Kcal/kg ideal body weight/d
Pentoxifylline Acriviadis E, Gastro 2000 119;1637-48 • PTX is a phosphodiesterase inhibitor which modulates the transcription of the TNFα-gene, lowers blood viscosity and reduces portal hypertension. • RCT • 101 patients with severe alcoholic hepatitis (mDF>32). • Given 400mg tds for 28 days vs placebo • Mortality 24% vs 46% at 28 days • Significant reduction in hepatorenal syndrome
Corticosteroids • Prednisolone 40mg/day for 28 days with a 20mg taper • Evaluated in 13 RCT’s • Evaluated in at least 4 Meta Analyses • Results are confounded by methodology. Cohen SM APT 2009 March (Review) • Cochrane review 2008 of 15 trials. • If take low bias trials • survival benefit for prednisolone in patients with severe alcoholic hepatitis (mDF>32) Rambaldi A APT 2008;27:1167-78
Corticosteroids • Mathurin P et al 2002 J Hepatol • Data from the 3 largest trials Pred vs. placebo • Analysed patients with mDF ≥ 32 • 28 day survival 85% vs 65% • NNT 5 • 2008, 5 largest trials reanalysed- confirmed the survival benefit Mathurin P, Hepatology 2008:48;635A
Corticosteroids • If the patient has severe alcoholic hepatitis mDF>32, MELD >11, GAHS>8 • Therapeutic trial of prednisolone 40mg PO • 7 days • If no improvement in bilirubin then discontinue Mathurin P Hepatol 2003;38;1363-9 Louvet A Hepatol 2008;45:1348-54
Conclusion • Severe alcoholic hepatitis is life threatening • The GAHS is clinically useful and more accurate than mDF and MELD at predicting outcome • If the patient has severe alcoholic hepatitis (GAHS>8, mDF>32) consider starting prednisolone 40mg/d • Reassess after 7 days • The results with pentoxifylline need corroboration in further trials
The End “All right, let's not panic. I'll make the money by selling one of my livers. I can get by with one “ Doh!
Corticosteroids RCT’s using Pred 40mg or equivalent for 28 days have been shown to increase both short and long term survival for patients with severe alcoholic hepatitis Mortality % 1mo 2mo 1yr 2yr Meta analyses: In support: Imperiale T, Ann Int Med 1990 ;113:299-307 Poynard T, Hepatology 1991;14:234A Raymond MJ, NEJM 1992 ; 26:507-12 Mathurin P, J Hepatol 2002; 36:480-7 Equivocal: Christiansen E, Gut 1995; 37:113-8