Download
1 / 45
490 likes | 826 Views
2011 Annual Membership Meeting. SPEECH & SWALLOWING. Anne G. Lefton, M.A. / CCC-SLP Nancy Sedat & Associates. “It feels like there’s something stuck in my throat!”. Swallowing. Transference of material from:. 3 Phases of Swallowing. Oral Pharyngeal Esophageal. Normal Swallow Sequence.

E N D
2011 Annual Membership Meeting SPEECH & SWALLOWING Anne G. Lefton, M.A. / CCC-SLP Nancy Sedat & Associates
Swallowing • Transference of material from:
3 Phases of Swallowing • Oral • Pharyngeal • Esophageal
Normal Swallow Sequence • In the mouth: • lips, teeth and tongue help prepare bolus (food mass) for further stages of swallowing. Lips Teeth Tongue Bolus
Normal Swallow Sequence • Access between the nasal cavity and mouth closes as bolus moves into pharynx (throat). Nasal Cavity Pharynx Bolus
Normal Swallow Sequence • Bolus is propelled esophagus • As esophagus entrance opens: Epiglottis helps guard against access to the lungs. Epiglottis Vocal Cords Trachea/Airway to the Lungs Esophagus Entrance
Normal Swallow Sequence • The airway reopens and the esophagus entrance closes as muscle contractions move bolus toward stomach. To the Stomach
Swallowing Disorders / Dysphagia • Oral Stage • Difficulty controlling, forming, or transporting a cohesive bolus
Swallowing Disorders / Dysphagia • Pharyngeal Stage • Pooling or Stasis • Aspiration Illustrations by Elliot Sheltman from Follow the Swallow by Jo Puntil-Sheltman
Evaluation of Swallowing Function • Non-instrumental clinical evaluation • Instrumental assessment • Modified Barium Swallowing Study (MBSS) • aka: Videofluoroscopic Swallowing Examination • Fiberoptic Endoscopic Evaluation of Swallowing (FEES)
Complications from Dysphagia • Pneumonia • Risk increases as dysphagia worsens • Choking • Longer Meal Times • Malnutrition • Dehydration • Weight Loss • Quality of Life • Loss of social interaction associated w/ eating
What to Do? • Immediate remedies: • If coughing/choking, never inhibit cough • Heimlich Maneuver • Stack breathing • Portable suction • CoughAssist device[www.respironics.com] • CoughAssist™Mechanical In-Exsufflator
Safe Swallowing Strategies • Swallowing techniques • Don’t talk with mouth full • Repeat swallows • Alternate solids and liquids • One sip at a time • Sip ‘n’ tip straws • Smaller bites • Slowed rate • Supervision and cueing • Smaller, more frequent meals per day
Safe Swallowing Strategies [cont.] • Changes in food & liquid consistencies • Avoid problem textures and consistencies • Gel/powder liquid thickener • Diet Hierarchy • Steak consistency diet • Pot roast consistency diet • Meat loaf consistency diet • Pudding consistency diet • Cream consistency diet (tube feedings)
Safe Swallowing Strategies [cont.] • Positioning • Chin tuck • Behavioral changes • Reduce distractions • Eat more calories early in the day or when there is less fatigue
Safe Swallowing Strategies [cont.] • Pill management • Take with applesauce, yogurt, pudding, ice cream, or any other slippery medium • Cool Whip! • Long-necked bottles • Carbonated beverages • Crush with pharmacist’s consent
Feeding Tubes • G-tube goes into stomach through an opening in skin
Feeding Tubes [cont.] • What it does: • Provides nutrition via an alternate route • Allows one to receive required nutrition and hydration when no diet texture can be swallowed safely or when oral feeding is not meeting nutritional / hydration needs • Allows for the combination of oral eating for pleasure and tube feeding for fluids and calories
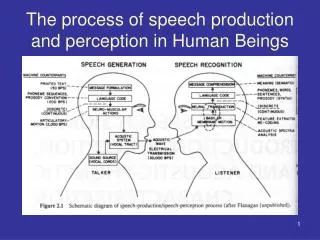
Speech • “Normal” sounding speech requires perfect coordination of the following systems: • Articulatory system (e.g., lips, tongue, etc.) • Resonatory system (e.g., velum/soft palate) • Phonatory system (e.g., vocal cords) • Respiratory system (e.g., lungs)
Random Speech Facts… • Approx. 14 different sounds produced every second when we verbalize. • Over 100 different muscles coordinate during speech.
“Its Greek to Me” • Ataxia comes from: • Greek word for “lack of order”
Ataxic Dysarthria • Disorder of sensorimotor control for speech production that results from damage to cerebellum or to its input and output pathways
Effects of Ataxia on Speech • Articulation: disruption of the timing, force, range, and direction of movements. • Imprecise consonant articulation • Distorted vowels • Breakdown is most evident during longer strings of speech
Effects of Ataxia on Speech [cont.] • Resonance: • Hypernasality • Hyponasality • May occur due to timing errors between the muscles of the velum and the other muscles of articulation. Soft Palate / Velum
Effects of Ataxia on Speech [cont.] • Phonation: the sound of the voice • Harsh vocal quality • due to decreased muscle tone • Vocal tremor
Effects of Ataxia on Speech [cont.] • Respiration: • Uncoordinated movements of the respiratory muscles • Exaggerated movements • Excessive loudness • Paradoxical movements (different muscle groups work against each other) • Talking too quickly • Decreased vocal volume • Trying to talk on residual air
Most Common Speech Changes • Imprecise consonants • Excess and equal stress • Articulatory breakdown • Distorted vowels • Harsh vocal quality • Mono pitch/Mono loudness • Slowed speech rate
What to do about it… • 1. Evaluation by a Speech-Language Pathologist • 2. Treatment • Exercises will target the affected system(s) • Improve breath support and coordination of breathing and speaking • Rate control techniques (e.g., finger/hand tapping to set the pace of appropriate syllable production) • Increase articulatory accuracy: over-articulate • Develop stress and intonation skills to regulate pitch and loudness
Compensatory Strategies For the Speaker... • Energy conservation • Minimize environmental noise/distractions • Establish context of message • Alter your rate of speech…SLOW it down. • Exaggerate articulation of final consonants in words • Use gestures/point to props • Boil down the message • decrease “filler” words • Keep important/key words
Compensatory Strategies For the Communication Partner… • Ascertain patients preferred strategy when not intelligible • Decrease the need for repetition fatigue and frustration • Ask yes/no questions • Know the topic • Maintain eye contact • Give undivided attention • Don’t interrupt or finish sentences • Let the speaker know the parts of the message you did not understand so s/he will not have to repeat the entire message. • Patience
Augmentative/Alternative Communication (AAC) • Low tech • Communication board • Alphabet board • Phrase board • High tech • Speech generating devices • An SLP can help explore your options • Other • Voice amplification • Chattervox OR SoniVox
Take Home Message With regard to speech or swallowing, there is always a way to keep you functioning at the highest level possible.
2011 Annual Membership Meeting THANK YOU! Anne G. Lefton, M.A. / CCC-SLP Nancy Sedat & Associates
References • Freed, D. (2000). Motor speech disorders diagnosis and treatment. San Diego, CA: Singular Thomson Learning, 2000. • Puntil-Sheltman, J. (1997). Follow the swallow. Seal Beach, CA: Sheltman Publishing, 37-40. • Rangamani, G.N., J. (2006). Managing speech and swallowing problems: A guidebook for people with ataxia. National Ataxia Foundation, 1-60. • Yorkston, K.M., Beukelman, D.R., & Bell, K. (1988). Clinical management of dysarthric speakers. San Diego, CA: College-Hill Press.