Download
1 / 8
80 likes | 86 Views
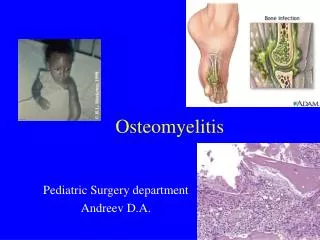
Osteomyelitis in the pediatric population is most often the result of hematogenous seeding of bacteria to the metaphyseal region of bone.

E N D
9111464959https://www.drgauravjain.com Dr Gaurav Jain 20 B Sainath Colony , Indore
What is Osteomyelitis? • Osteomyelitis in the pediatric population is most often the result of hematogenous seeding of bacteria to the metaphyseal region of bone. • Diagnosis is generally made with MRI studies to evaluate for bone marrow edema or subperiosteal abscess. • Treatment is nonoperative with antibiotics in the absence of an abscess. Surgical debridement is indicated in the presence of an abscess.
What Causes Osteomyelitis? • Pathophysiology • Staph aureus • is the most common organism in all children • strains of community-acquired (CA) MRSA have genes encoding for Panton-Valentine leukocidin (PVL) cytotoxin • PVL-positive strains are more associated with complex infections, multifocal infections, prolonged fever, abscess, DVT, and sepsis • MRSA is associated with an increased risk of DVT and septic emboli • Group B Strep • is most common organism in neonates • Kingellakingae • becoming more common in younger age groups • Pseudomonas • is associated with direct puncture wounds to the foot • H. influenza • has become much less common with the advent of the Haemophilus influenza vaccine • Mycobacteria tuberculosis • children are more likely to have extrapulmonary involvement • biopsy with stains and culture for acid-fast bacilli is diagnostic • Salmonella • more common in sickle cell patients
What are Factors for Osteomyelitis? • Risk factors • diabetes mellitus मधुमेह • hemoglobinopathy हीमोग्लोबिनोपैथी • juvenile rheumatoid arthritis गठिया • chronic renal disease गुर्दे की बीमारी • immune compromise प्रतिरक्षा की कमी • varicella infection संक्रमण • Mechanism • local trauma and bacteremia lead to increased susceptibility to bacterial seeding of the metaphysis • history of trauma is reported in 30% of patients • Incidence • 1 in 5000 children younger than 13 years old 13 साल से कम उम्र के 5000 बच्चों में से 1 • Demographics • mean age 6.6 years औसत आयु 6.6 वर्ष • 2.5 times more common in boys लड़कों में 2.5 गुना अधिक आम • more common in the first decade of life due to the rich metaphyseal blood supply and immature immune system पहले दशक में अधिक • not uncommon in healthy children स्वस्थ बच्चों में असामान्य नहीं
What is treatment of Osteomyelitis? Nonoperative treatment • antibiotic therapy alone • indications • early disease with no subperiosteal abscess or abscess within the bone • surgery is not indicated if clinical improvement obtained within 48 hours • modalities • antibiotics • begin with empiric therapy • generally, nafcillin or oxacillin, unless high local prevalence of MRSA (then use clindamycin or vancomycin) • mechanism of action for vancomycin involves binding to the D-Ala D-Ala moiety in bacterial cell walls • if gram stain shows gram-negative bacilli — add a third generation cephalosporin • convert to organism-specific antibiotics if organism identified • mycobacterium tuberculosis • treatment for initial 1 year is multiagent antibiotics and rarely surgical debridement due to risk of chronic sinus formation • duration • typically treat with IV antibiotics for four to six weeks, आम तौर पर चार से छह सप्ताह के लिए IV एंटीबायोटिक दवा दी जाती है • controversial duration • intravenous versus oral • often a case by case decision with input from infectious disease consultation
surgical drainage, debridement, and antibiotic therapy • indications • deep or subperiosteal abscess हड्डी में मवाद का इक्कठा होना • failure to respond to antibiotics एंटीबायोटिक दवाओं का जवाब देने में विफलता • chronic infection जूना / पुराना संक्रमण • contraindications • hemodynamic instability, as patients should be stabilized first — however sometimes operative treatment of the underlying infection helps stabilize the patient
Contact Dr Gaurav Jain • 20 B Sainath Colony , Indore • 9111464959 • https://www.drgauravjain.com