Download

1 / 48
540 likes | 1.2k Views
Schistosomiasis. -07— 28-7-2015 Dr.jagadeesh (P.G) . The sweetest pairs in the world. Class Trematoda (Flukes). Leaf shaped, unsegmented flat worms with a size ranging from 1 mm to several cms

E N D
Schistosomiasis -07—28-7-2015 Dr.jagadeesh (P.G)
Class Trematoda (Flukes) • Leaf shaped, unsegmented flat worms with a size ranging from 1 mm to several cms • Organs of attachment – 2 strong, muscular cup shaped suckers (oral & ventral) • Hermaphrodites except for the schistosomes • Oviparous (lay eggs)
Classification of trematodes • Intestinal fluke -> Fasciolopsis buski • Liver fluke -> Fasciola hepatica, Clonorchis sinensis • Lung fluke -> Paragonimus westermani • Blood flukes -> • In the vesical (bladder)venous plexus – Schistosoma haematobium • In the sigmoido-rectal venous plexus – S.mansoni • In the ileo-cecal venous plexus – S.japonicum
Known as blood flukes • Cause schistosomiasis ,the second most common tropical parasitic disease . • Affect more than 200 million people . • Order---Strigeda • Superfamily--- Schistisomatoidea • Family---Schistosomatidae
Schistosomiasis, Bilharziasis • Parasitic disease caused by several species of flatworm • Affects many in developing countries (it’s estimated that 200 Millions have the disease and that of those, 120M are symptomatic) • Can contract it by wading or swimming in lakes, ponds and other bodies of water infested with the parasite’s snail host.
A Brief History... • First described by German pathologist Theodore Maximilian Bilharz • Bilharz performed autopsies on Egyptian patients who had died from the disease: found male & female parasite eggs in the liver portal system, bladder. • Later seen in Japan, called Katayama fever • Symptoms: rash on legs, fever, diarrhoea, bloody stools emaciation, edema death.
Classification • Phylum: Platyhelminthes (flatworms) • Subclass: Digenea (alt. gen. seen in life cycle) • Order: Strigeida • Family: Schistosomatidae (blood flukes) • Subfamily: Schistosomatinae • Genus: Schistosoma • Species: S. mansoni S. japonicum S. haematobium S. indicum
General charecteristics • General morphology same as other trematodes • Adult worm— Resides in venous plexuses cylindrical,covered with thick tuberculated and syncycial tegument except S.japonicum • No muscular pharynx ,intestinal caeca reunite to form single canal. • Sucker armed with delicate spines . • Sex separate female long and slender than male. • Male poses a gynecophoric canal on ventral side of which female repose.
Male has 4 to 9 testes • Humans are definitive host • Snails are intermediate host • No second intermediate host • Egg--non operculated with a spine like projection , Eggs are fully embryonated when excreted that hatch to form meracidum • Larva---various forms are miracidium ,sporocyst and cercaria • No radiae and metacercaria stage ,Cercaria are fork tailed and are infective form to man.
Schistosoma Haematobium • Causes urinary schistosomiasis or bilharziasis • Adult male holds the female worm in gynecophoric canal and resides in venous plexus of urinary bladder and ureter. • India cases are rare (Rathnagiri district ) . • Adult—diecious,live for 20-30 years. Male-15mm x 0.9mm,4-5 testes .Female-20 mm x 0.25 mm,fertilized female contains 200 terminally spined eggs • Egg—120 um x 40 um,oval,brownish yellow and non operculated have terminal spine . • Larva—miracidium ,sporocyst and cercaria
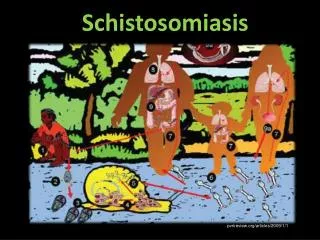
Life cycle • Man definitive host and fresh water snail intermediate host. • Man acquires infection by penetration of skin by the infective form present in contaminated water. • Development in man—Free swimming infective cercaria---penetrate intact epidermis—loses tail and outer coating----next stage larva---schistosomula---via dermal vein----lung ----via systemic circulation—portal circulation –in liver sinusoids feed and develop into adult worm---become sexually active—pair—migrate against blood stream to vesical and ureteric venous pluxses
Young fluke—coated with host red cell antigen and histocompatibility antigen—so not recognised as foreign and escape host IR. • Fertilized female lays eggs in these plexuses—eggs penetrate venules and urinary mucosa with help of terminal spines and lytic substances—eggs along with blood exccreted in urine. • Pre-patent period---time b/w-penetration of cercaria and first production of eggs(2-3months)
Development in water—fully embryonated eggs are passed in urine gain access into water—hatch to release free swimming miracidium • Development in snail---miracidium live in water for 8-12 hours and infect snail of genus Bulinus---miracidium multiply asexually---1st and 2nd generation sporocyst---transform to fork tailed cercaria • Single miracidium can give rise to 105 cercaria—escape from snail into water and cause human infection
Pathogenesis • Acute scistosomiasis---skin invasion by cercaria causes dermatitis at penetration site---allergic papular lesion • Migration of schistosomula in lungs– cough ,fever
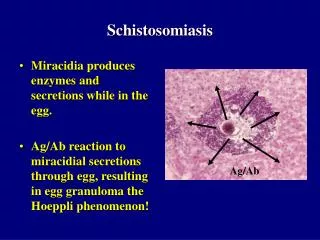
Chronic Infection(Late) • Symptoms of chronic infection caused by eggs that travel to various parts of body usually develops after 3-6 months • Pathogencity is due to egg deposition. • Eggs passing into UB cause mucosal damage---dysuria and hematuria • Soluble antigens released from eggs provoke DHT reaction around them---lead to formation of egg granuloma composed of egg at the center surrounded by macrophages ,lymphocytes, fibroblasts and multinucleated giant cells. • Granuloma differ in size---join to form larger nodules—urinary mucosa covering the nodules show glandular metaplasia (cystic glandularis )
In chronic stage—fibrotic changes occur visible as sandy patch in cystoscope. • Obstructive uropathy—fibrosis may cause obstruct lower end of ureter ---hydroureter and hydronephrosis—may be seen in 25-50% infected children • Bladder carcinoma---metaplastic changes in urinary mucosa may lead to Carcinoma bladder Predisposing factors—nitroso comps intake, secondary bacterial infection Type--- squamous cell carcinoma is most common (high worm burden) , transitional cell carcinoma.
Microscopic Detection—detection of non operculated terminally spined eggs in urine . The terminal haematuria blood portion collected b/w 12 pm and 3 pm concentrated by centrifugation or membrane filtration Diagnosis S. mansoni S. japonicum S. haematobium
Histopathology—demonstration of eggs in bladder mucosa by biopsy Antibody tests– usefulmin sero diagnosis –2 assay savailable to detect antibodies aginst S. haematobium adult worm microsomal antigen [HAMA] HAMA_FAST_ELISA—(falcon assay screening test enzyme linked immuno sorbent assay) HAMA_EITB-enzyme linkd immuno sorbent blot Cercarial huller reaction ,indirect fluorescent antibody test and indirect haemagglutination IgE and IgG-4 elevated
Antigen tests: -detection of circulating antigen in blood indicate recent infection and can be used for monitoring treatment Circulating cathodic antigen (CCA) and Circulating anodic antigen—in urine and serum by ELISA ELISA—using specific monoclonal antibody against Soluble egg antigen Molecular detection: 20-25% of schistosomiasis genome has been sequenced can use 2 probes to detect S. mansoni DNA in human blood Genome sequencing has the potential to yield DNA vaccines Diagnosis
S.mansoni • Cause intestinal schistosomiasis—resides in mesentric veins draining sigmoidorectal region • Adult worm similar to other schistosomes, non operculated eggs have lateral spines, fork tailed cercaria is infecting form . • Life cycle—similar to S.haematobium except—humans definitive host but some times monkey ,dog may act as reservoir and definitive host. intermediate host—Biomphalaria Adult live in mesentric veins draining sigmoidorectal junction
Pathogenesis and clinical feature Pathogensis occurs in 3 stages • Cervical dermatitis---after 2-3 days of cercarial invasion, an itchy maculopapular rash on affected area of skin called cervical dermatitis or swimmers itch .Cervical dermatitis is particularly severe in avian and mammalian schistosomiasis. Man being an aberrent host, these parasites don’t under go further development. This condition occurs when a person from non endemic area visits endemic area.Cercaria dies in skin and evoke severe allergic response
Katayama fever---acute schistosomiasis,occur within 4-8 weeks of infection,when schistosomes start laying eggs,Antigens released from eggs and adult worm stimulate host humoral response—lead to formation of immune complex and serum sickness like illness called katayama fever----fever,generalized lymphedinopathy and hepatospleenomegaly.Parasite specific antibodies are detected.High peripheral blood eosinophilia.
Chronic schistosomiasis—after eggs are produced they get trapped in small venules and are carried into the intestine and excreted in feces , some carreid to liver and other parts of body • Intestinal disease—eggs deposited in intestinal wall. Soluble antigen liberated from eggs induce inflammatory reaction that lead to granuloma formation around eggs in the intestine.Fibrosis and thickening occurs in intestinal wall along entire length of colon and rectum. • Hepatosplenic disease—granuloma formation and fibrosis in liver—symmers pipe stem fibrosis—impend portal blood flow—lead to PHT,hetatomegaly,spleenomegaly and gastric verices
Pulmonary involvement—eggs carried and lodgedin lung by collateral circulatio.egg sequestation and granuloma formation may cause pul. Emboli,PHT Rt Heart failure. • Spinal cord—myelopathy • Nephrosclerosis and Renal failure—due to circulating immune complex deposition on basement membrane • Secondary bacterial infection.
Lab diagnosis Stool micro—acute cases eggs with lateral spines in stool. In chronic cases or patient on low worm load---multiple stool tests, stool concentration. Hatching test—hatching of motile miracidia when eggs are diluted in water and perpendicular beam of light is passed through the water at the top Quantification of eggs in stool—kato thick smear techique. Rectal biopsy—histopathological demonstration of eggs in biopsy material from rectal mucosa. Egg shell is acid fast stain y modified Z-N. Antigen and antibody dection.
S.japonicum • Most pathogenic species, resides in mesentric veins draining ileocecal. • Most commonly seen in Japan, China, chidren of 5-10 years of age affected • Adult similar to S.haematobium except ,bodu surface is smooth,eggs small and more sperical and has rudimentary lateral spine. • Life cycle—similar except definitive host is man and some times domestic animals,intermediate Oncomelania species , high egg out put-3000/day
Pathogenesis and clinical features • All most similar to S.mansoni more severe---high egg load and smaller size. • Cercarial dermatitis. • Katayama fever—after 40 days ,more severe ,may lead to death. • Intestinal disease—deposition of egg granuloma in intestinal wall--mucosal hyperplasia , ulcer,microabscess and some times pseudohpolyposis with blood loss. • Hepatosplenic disease • CNS infection-2-4%,parietal lobe—Jacksonian convulsions and grand mal seizures. • Carcinoma—colorectal and liver • Chronic sec infection—salmonella HBV
S.intercalatum—clinical features similar to S.mansoni. Eggs same as haematobium but large. • S.mekongi—in Mekong river bases of Laos ,all features similar to S.japonicum • Schistosomiasis in India—rare{absence of suitable int host,environmental condition and host IR. Confined endemic focus in Rathnagiri district. Cervical dermatitis and paddy field dermatitis noted
Treatment • Swimmer’s itch and Katayama Fever are usually treated symptomatically. • Chemotherapy is treatment of choice - Praziquantel is most widely used drug. Praziquantel • Extremely well tolerated, few side effects • Broad-spectrum antihelminthic drug (antihelminthic= drugs that expel parasitic worms) • Cures schistosomiasis in 80–90% of patients, 90% reduction in egg excretion in those not cured • Causes worm muscles contract – cannot hold onto human tissues • Resistance has been reported in Egypt and Senegal
Treatment Others: • Metrifonate against S. haematobium • Niridazole against S. japonicum • Oxamniquine against S. mansoni • WHO recently approved use of combo of 3 drugs at once (rule is always no more than 2) to cure a few related diseases (incl. Schistosomiasis) in hopes that eradication will be faster. Complications • Drugs ineffective when fibrosis has developed - treatment is then focused on managing the complications (e.g. portal hypertension) • Anticonvulsants may be needed in patients with CNS complications (S. japonicum).
Prevention • For travelers it’s easy- don’t swim in fresh, stagnant water (running water is better, still not safe). • Harder in endemic areas people are dependent on nearby freshwater. • Focused on education, eliminating snail nesting grounds • Molluscicides can be used to eliminate snails. • Proper irrigation systems and engineering are key • There are ways to build irrigation and canalization systems that don’t allow snails to inhabit the surrounding area • However, many irrigation/canalization projects since the 50s have ignored UN instructions, may have contributed to spread of the parasite
Vaccination • Humoural environment hostile to parasites, but eggs stay in blood for weeks without significant attack • Irradiated cercariae vaccine very effective in clinical trials. Delivery complications & difficulty in establishing proper safety standards make it problematic as human vaccine. • Currently testing combination-protein and combination DNA vaccines but so far unsuccessful. Some issues: • Co-evolution: disease has existed since 4000 BC – has developed ways to evade human immune responses. • Antigen sharing - we share a number of antigens with the parasite; difficult to create vaccine that doesn’t cross-react with our own cells. • Evidence suggests that our immune response actually helps mature female lay eggs
Discussion Why isn’t there a vaccine yet? • What factors make vaccine development difficult? • Should we focus on vaccine development and if so, who should shoulder the cost? • Some have argued that wide-scale treatment of schistosomiasis should not be a priority- what factors can affect this decision? Since the 1950’s, specifications and design criteria have been made available by the United Nations (UN) which show how dams, irrigation schemes, and similar projects an be constructed so that they are not suitable habitats for the snails and also make it more difficult for the local population to come into contact with the water. Unfortunately, many projects have been completed without taking these specifications and design criteria into account. Q: Should we put more emphasis on this?