Download

1 / 22
220 likes | 297 Views
Open-Versus Closed-Kinetic Chain Exercise in Rehabilitation. Rehabilitation Techniques for Sports Medicine and Athletic Training William E. Prentice. Introduction. Closed Kinetic Chain (CKC): effective technique of rehabilitation Particularly with injuries involving the lower extremity

E N D
Open-Versus Closed-Kinetic Chain Exercise in Rehabilitation Rehabilitation Techniques for Sports Medicine and Athletic Training William E. Prentice
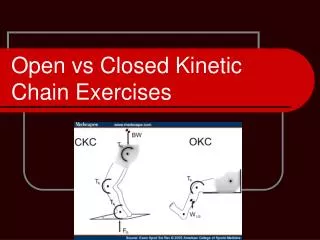
Introduction • Closed Kinetic Chain (CKC): effective technique of rehabilitation • Particularly with injuries involving the lower extremity • Ankle, knee and hip constitute the kinetic chain of lower extremity • When distal segment of lower extremity is fixed/stabilized or weight bearing it is considered Closed • Will involve fixed joints with mobile joints in between
Introduction • Open Kinetic Chain (OKC): distal segment is mobile or not fixed • Isolated joint exercise. i.e.. Seated leg extension • Most Upper extremity movements in sports are open chain with the hand moving freely
Concept of Kinetic Chain • Closed Link system: each moving body segment receives force from and transfers force to, adjacent body segments • Movement and one joint produce predictable movement at all other joints • Muscle recruitment and joint movements are different than when distal segment moves freely in OKC ex. • Concurrent shift: Concentric and eccentric contractions at opposite ends of a muscle during CKC movement • For example: during squat to stand the hip and knee both extend and the rectus femoris shortens at the distal end and lengthens at the proximal end • Functional action that cannot be reproduced during isolated OKC ex.
Advantages and Disadvantages of OKC vs. CKC Exercises • Choice to use one or the other depends on desired treatment goal • Characteristics of CKC: • Increased joint compressive forces • Increased joint congruency (stability) • Decreased shear forces • Decreased acceleration forces • Stimulation of proprioceptors • Large resistance forces • Enhanced dynamic stability
Advantages and Disadvantages of OKC vs. CKC Exercises • OKC characteristics: • Increased acceleration forces • Decreased resistance forces • Increased distraction and rotational forces • Increased deformation of joint and muscle mechanoreceptors • Greater shear forces • Great moment forces (1 joint in motion) • Isolation exercise use contraction of specific muscle or muscle group that produces single plane or occasionally multiplanar movement
Advantages and Disadvantages of OKC vs. CKC Exercises • Biomechanical Perspective: • CKC : safer and produce stresses and forces that are potentially less of a threat to healing structures • Co-contraction of agonist and antagonist must occur during normal movements to provide joint stabilization • Decrease shear forces seen in OKC that may damage soft tissue structures that are healing • Increase joint compressive forces will further enhance joint stability • CKC more functional than OKC: most sport related activity and activities of daily living involve CKC of lower extremity
Advantages and Disadvantages of OKC vs. CKC Exercises • Biomechanical Perspective • OKC: isolated to single joint • Beneficial to improve strength and increase ROM at specific joint • Correct strength deficits of specific muscles or joints and beginning of rehabilitation when athlete not able to perform CKC exercises • Loss of ROM, pain or swelling may not allow athlete to perform CKC exercises
CKC to regain NM Control • Coordinated movement is controlled by CNS that that integrates input from joint and muscle mechanoreceptors acting within kinetic chain • CKC Exercises that act to integrate all of the functioning elements would seem to be most appropriate • CKC recruit foot, ankle, knee and hip muscles that reproduce normal loading and movement forces in all joints • Reestablish joint position sense and proprioception through facilitation of proprioceptive feedback
CKC Exercises for LE • Biomechanically shock absorption, foot flexibility, foot stabilization, acceleration and deceleration, multiplanar movement and joint stabilization must occur in all joints of LE for normal function to occur • Foot shock absorber and force producer through normal ambulation (gait) • OKC exercises produce a lot of shear force on tibiofemoral (knee) joint • Co-contraction of hamstring or CKC exercises reduces shear force • OKC exercises produce a lot of compressive forces on PTF joint • CKC exercises decreases contact stress by increasing contact area on femur
CKC Exercises for LE • Mini squats • Wall slides • Lunges • Step ups • Fwd. & Lateral • Leg Press • Stationary Bicycle • TKE • Trampoline • BAPS • Sideboard
OKC vs. CKC in Upper Extremity • UE most functional as OKC system • Hand moves freely • Dynamic movement • High velocity • Proximal segment of UE used as stabilization as distal segments have high degrees of mobility
OKC vs. CKC in Upper Extremity • CKC in UE: • Strengthening and neuromuscular control of shoulder girdle stabilizers and core • Co-contraction and muscle recruitment in early stages of rehab to prevent shutdown of rotator cuff • Scapular stabilizers and Rotator Cuff control movement about shoulder • Provide stabile base for more mobile and dynamic movements at distal end • Promote and enhance dynamic joint stability • Resistance axially or rotationally • Joint compression and approximation acts to enhance muscular co-contraction about the joint producing dynamic stability
OKC vs. CKC in Upper Extremity • OKC Exercises in UE: • Essential to regain high velocity dynamic movement of shoulder, elbow, wrist and hand • CKC and OKC should both be used in rehab to stabilize and build muscular strength and endurance in upper extremity
OKC vs. CKC in Upper Extremity • Weight shifting • Standing, quadruped, tripod, stable, unstable and movable surfaces • Push ups • Press ups • Step ups • Slideboard • Push up with rotation
PNF Exercises for Strength and Endurance • Uses proprioceptive, cutaneous and auditory input to produce functional movement • First used to treat patients with paralysis or other neuromuscular disorders • Since 1970’s used in rehabilitation to increase strength, range of motion and flexibility • Used to decrease deficiencies in strength , flexibility, and neuromuscular coordination in response to demands that are placed on NM system
PNF Exercises for Strength and Endurance • Emphasis on selective re-education of individual motor elements through development of NM control, joint stability and coordinated mobility • Each movement learned and reinforced through repetition • Holistic, integrating sensory, motor, and psychological aspects of rehabilitation • Incorporates reflex activities from spinal level and upward, either inhibiting or facilitating them as appropriate
Basic Principles of PNF • Patient taught patterns from starting to terminal position • Verbal and physical cues, brief and simple • Patient watches moving limb for visual feedback for directional and positional control • Manual contact with appropriate pressure is essential • Firm and confident • Manner in which AT touches patient will facilitate movement • Proper body position and mechanics of AT in line with movement patterns • Amount of resistance should facilitate maximal response and smooth coordinated movement
Basic Principles of PNF • Rotational movement is critical component because maximal contraction is impossible without it • Distal movement occurs first: • Quick stretch before muscle contractions facilitates a muscle to respond with greater force
Basic strengthening techniques • Rhythmic initiation • Repeated contraction • Slow reversal • Slow reversal hold • Rhythmic stabilization
PNF patterns • Human movement rarely involves straight motion because all muscles are spiral in nature and lie in diagonal directions • PNF patterns are diagonal and rotational movements • Three components • Flexion-extension • Abduction-adduction • Internal rotation-external rotation
PNF Patterns • Figures 14-1 and 14-30 in text • Rule of 30’s