Download
1 / 61
610 likes | 779 Views
EXPOSURE TO ULTRAVIOLET (UV) LIGHT. Sophie J. Balk, M.D. Professor of Clinical Pediatrics Albert Einstein College of Medicine NEETF Children’s Environmental Health Faculty Champions Initiative. www.charlie.org. GOALS: TO DISCUSS. Background on UV radiation (UVR) Health effects

E N D
EXPOSURE TO ULTRAVIOLET (UV) LIGHT Sophie J. Balk, M.D. Professor of Clinical Pediatrics Albert Einstein College of Medicine NEETF Children’s Environmental HealthFaculty Champions Initiative
GOALS: TO DISCUSS.. • Background on UV radiation (UVR) • Health effects • Focus on skin cancer • Prevention messages • What to ask in the history • Resources
UVR MODIFIED BY PASSAGE THROUGH ATMOSPHERE…. • Stratosphere (10 - 50 Km above sea level) • Absorption by ozone • Scattering by molecules • Troposphere (0 -10 Km above sea level) • Absorption by pollutants • Scattering by particulates • Clouds
INCREASED UV INTENSITY... • At midday • In summer • Closer to the equator • At higher altitudes • Reflected from ground surfaces, sand, snow, water
HEALTH EFFECTS OF UVR • Skin • Eyes • Immune system AAP Pediatric Environmental Health, November 2003.
EFFECTS ON THE SKIN • Vitamin D Production • Erythema and sunburn • Tanning • Skin aging • Photosensitivity • Non-melanoma skin cancer • Basal cell carcinoma • Squamous cell carcinoma • Melanoma AAP Pediatric Environmental Health, November 2003.
ERYTHEMA & SUNBURN • Minimal erythemal dose (MED) depends on • Skin type and thickness • Amount of melanin and ability to produce melanin after exposure • Intensity of the radiation • Six sun-reactive skin types
TANNING • Protective response to sun exposure • Immediate tanning: Induced by UV-A, no new melanin • Delayed tanning: Induced by UV-B, begins at 2-3 days, peaks at 7-10 days, new melanin formed
NON-MELANOMA SKIN CANCER (NMSC) • Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) • Most common malignancies in adults: > 1,000,000/year • Found on maximally-exposed areas • Usually not fatal unless untreated • Related to cumulative sun exposure American Cancer Society 2006 ( www.cancer.org). Accessed 6-28-06.
MELANOMA • Most common fatal skin cancer • 2006: 62,190 new cases with 7,910 deaths1 • Occurs in teens, young adults • Metastatic melanoma has a grave prognosis • Prevention, early detection are key 1 – American Cancer Society 2006 (www.cancer.org). Accessed 6-28-06.
MELANOMA IN YOUNG ADULTS AND CHILDREN • A common malignancy in whites1 • 2nd most common, women 20 – 29 • 3rd most common, men 20 - 29 • Melanoma in children2 • Incidence rising • 33 patients < 14; 25 yr experience • Presentation often atypical: most lesions raised, well-defined borders • Lesions unlike any other on child 1 - Wu et al. Cancer Causes and Control 2005; 2 - Ferrari et al, Pediatrics 2005
MELANOMA A - Asymmetry B - Border C - Color D - Diameter E - Evolving
MELANOMA • Lifetime risk • 1930: 1 in 1500 • 1987: 1 in 120 • 2002: 1 in 681 • 2010: 1 in 501 1- Rigel DS. Dermatol Clin 2002; 20
WHY IS THE INCIDENCE OF MELANOMA RISING? • Thought to be related to sun exposure • Depletion of the ozone layer • Changing patterns of dress • More leisure time • “Sun culture” Pediatric Environmental Health. AAP 2003
SUNLIGHT AND MELANOMA • Epidemiologic and biological evidence implicate sunlight in the pathogenesis of melanoma Pediatric Environmental Health. AAP 2003
SUNLIGHT AND MELANOMA • Latitude • Race and pigmentation • Childhood exposure • Nevi Pediatric Environmental Health. AAP 2003
CHILDHOOD EXPOSURE • ~25% of lifetime sun exposure occurs during childhood and adolescence1 • Episodic high exposures sufficient to cause sunburn, particularly in childhood and adolescence, increase the risk of melanoma2 1- Godar et al. Photochem Photobiol 2003 2 -Elwood, Jopson. Int J Cancer 1997;73
CHILDHOOD EXPOSURE • Migration studies: High sun exposure during childhood is important in the pathogenesis of melanoma1 1 - Khlat et al. Am J Epidemiol. 1992;135
NEVI • Acute sun exposure is implicated in the development of nevi in children1 • There is a relationship between the number and type of nevi and the development of melanoma1 • Dysplastic nevi: precursor lesions that increase risk2 1 – Gallagher et al. Arch Dermatol. 1990; 126 2 - Clark. Arch Dermatol. 1988;124
BIOLOGIC EVIDENCE • UVB exposure DNA lesions (pyrimidine dimers) whose incomplete repair leads to mutations1 • UVA causes oxidative damage to DNA mutations1 • UVR contributes to immune suppression2 1 - Gilchrest et al. N Engl J Med. 1999;340 2 – Strickland, Kripke. Clin Plast Surg. 1997;24
BIOLOGIC EVIDENCE: XP • Xeroderma pigmentosum (XP): Grossly deficient repair of DNA damaged by UVR1 • SCC, BCC and melanoma seen beginning at young ages1 1 - Photosensitivity. In Behrman, Kliegman, Jenson, eds. Nelson Textbook of Pediatrics. 16th ed. Philadelphia, PA: WB Saunders Co; 2000:1998-2001
SUN PROTECTION • Sun protection is recommended to prevent skin cancer, including melanoma • Sun protection is recommended beginning early in life • Pediatric clinicians may play an important role in delivering messages Pediatric Environmental Health. AAP 2003
PREVENTION AT ALL DEVELOPMENTAL STAGES • Infants • Lack mobility • Skin has less melanin than at any other time • Children • New patterns of exposure • Adolescents • Susceptible to society’s ideas about beauty and health
UV LIGHT – PREVENTION MESSAGES • Do not burn; avoid sun tanning and tanning beds • Generously apply sunscreen • Wear protective clothing • Seek shade • Use extra caution near water, snow and sand • www.skincancerprevention.org/Tips/tabid/54/ Default.aspx
DO NOT BURN; AVOID SUN TANNING AND TANNING BEDS • Burning raises melanoma risk • Avoid/limit exposure during peak hours (10AM – 4PM) • Avoid intentional tanning
GENEROUSLY APPLY SUNSCREEN • Sunscreen is the sun protection method most commonly used1 • Apply to all exposed skin using SPF > 15 • Broad protection (UVA & UVB) • Reapply often 1 - Olson et al. Pediatrics 1997;99
WEAR PROTECTIVE CLOTHING • Simple, practical protection • The structure (weave) of the fabric is most important • Light-weight long pants and sleeves suggested • Hats with a bill or brim • Sunglasses
SEEK SHADE • Shade is useful but… • Shade offers insufficient protection because UV light is scattered and reflected • A fair-skinned person sitting under a tree can burn in an hour
SUNSCREENS • Came into use in 1950’s • Promoted tanning without burning • First true sunscreen (PABA) became available in 1970’s • High-intensity sunscreens within last 15 years Rigel DS. Dermatol Clin 2002; 20.
OPAQUE SUNSCREENS • Scatter, reflect, block UV light • Zinc oxide, titanium dioxide, red vetenary petrolatum, talc • Effective for diseases related to light exposure (SLE, XP, solar urticaria) • Useful for those spending extensive periods outside Rigel DS. Dermatol Clin 2002; 20.
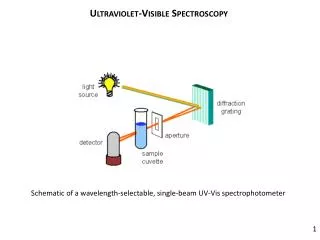
CHEMICAL SUNSCREENS UVB: 290 – 320 nm UVA: 320 – 400 nm Rigel DS. Dermatol Clin 2002; 20.
SUN PROTECTION FACTOR - SPF • Ratio of amount of time to sunburn with sunscreen compared to time to sunburn without sunscreen • 1970’s: SPF’s 2 – 4: 50 – 75% protection • High-potency sunscreens: SPF’s 15 – 50, 93 – 98% protection Rigel DS. Dermatol Clin 2002; 20.
LIMITATIONS OF SPF SYSTEM • Applies to UVB protection only • Measured under ideal conditions • Concerns about: • Using adequate amounts • Applying before needed • Need for frequent reapplication
SUNSCREEN AND MELANOMA • Sunscreen • Reduces sunburn • Can prevent actinic keratoses1 • Can prevent SCC2 • No conclusive data in humans to demonstrate that sunscreen prevents melanoma or BCC 1 - Thompson, Jolley, Marks. NEJM 1993; 329 2 – Green et al. Lancet 1999; 354
IS SUNSCREEN USE A RISK FACTOR FOR MELANOMA? • Swedish case-control study found increased risk1 • Several studies found increased risk with sunscreen use; some studies found decreased risk; others found no change2 1 – Westerdal et al. Melanoma Res 1995; 5:59-65. 2 - Cooper, Lim. J Amer Acad Dermatol 1999; 40.
IS SUNSCREEN USE A RISK FACTOR FOR MELANOMA? • No studies demonstrate that sunscreens are carcinogenic1 • Sunscreen users may extend their time out in the sun2 • There may be greater exposure to UVA1 1-Cooper, Lim. J Amer Acad Dermatol 1999; 40 2-Autier et al. J Natl Cancer Inst. 1999;91:1304-1309
SUNSCREEN MAKERS SUED FOR MISLEADING CLAIMS • April 2006: 9 suits involving popular brands charged that manufacturers inflated claims about sunscreens’ protection • Sunscreen called the “snake oil of the 21st century“ • Focus on labels claiming equal UVA/UVB protection; “all day”; “waterproof”; www.consumeraffairs.com/news04/2006/03/sunscreen.html. Accessed 7-29-06
RECOMMENDATIONS • AAP, ACS, AAD, EPA, CDC, others recommend multi-component message • Sunscreen is one part of a sun protection program • Sunscreen should not be used to extend time spent in the sun
SUNSCREEN AND VITAMIN D METABOLISM • Vitamin D produced in the skin by action of UVB • Inadequate sunlight is an important risk factor for rickets • Concerns that sunscreen use may affect levels of Vitamin D
SUNSCREEN AND VITAMIN D METABOLISM • AAP policy - April 2003 • Infants need 200 IU Vit D/day • Human milk: < 25 IU/L Vit D • Infant formula: 400 IU/L Vit D • Supplementation: all breast-fed infants, formula-fed infants taking <500 ml/day, children with inadequate intake/sun AAP Section on Breastfeeding and Committee on Nutrition. Pediatrics 2003; 111.
VITAMIN D AND CANCER PREVENTION • Recent studies suggest a role for vitamin D in cancer prevention • Colon, breast, prostate, lung • High prevalence of vitamin D deficiency/insufficiency • Insufficient evidence to make recommendations about sun exposure http://msnbc.msn.com/id/7875140/print/1/displaymode/1098. Accessed 7-04-06