Download
1 / 64
690 likes | 1.11k Views
Electrolyte Imbalance and Acid-Base disorders. Victor Politi, M.D., FACP, Medical Director, St. John’s University Dr. Andrew J. Bartilucci Center College of Pharmacy and Allied Health Professions, PA Program. Importance of Homeostasis.

E N D
Electrolyte Imbalance and Acid-Base disorders Victor Politi, M.D., FACP, Medical Director, St. John’s University Dr. Andrew J. Bartilucci Center College of Pharmacy and Allied Health Professions, PA Program
Importance of Homeostasis • Fluid and electrolyte and Acid-base balance are critical to health and well-being • Maintained by intake and output • Regulation by renal and pulmonary systems
Imbalances Result From: • Illness • Altered fluid intake • Prolonged vomiting or diarrhea
Distribution of Body Fluids • Water is the largest single component of the body • 60% of adult’s weight is water • Healthy people can regulate balance
Composition of Body Fluids • Water • Electrolytes • Separates into ions when dissolved • Carries an electrical charge • Positive charge – CATIONS • Sodium, Potassium, Calcium • Negative charge – ANION • Bicarbonate, Chloride
Fluid Intake • Regulated primarily by thirst mechanism • In the hypothalamus • Osmoreceptors monitor serum osmotic pressure • Hypothalamus stimulated when osmolarlity increases • Thirst mechanism stimulated • With decreased oral intake • Intake of hypertonic fluids • Loss of excess fluid • Stimulation of renin-angiotensisn-aldosterone mechanism • Potassium depletion • Psychological factors • Oropharyngeal dryness
Fluid Intake (cont) • Average adult intake • 2200-2700 cc/day • Oral – 1100-1400 • Solid foods – 800-1000 • Oxidative metabolism – 300 • By-product of cellular metabolism of ingested foods
Fluid Intake (cont) • Must be alert • Able to perceive mechanism • Able to respond to mechanism • **At risk for dehydration: • Elderly • Very young • Neurological disorders • Psychological disorders
Fluid Output Regulation • Kidneys • Major regulatory organ • Receive about 180 liters of blood/day to filter • Produce 1200-1500 cc of urine • Skin • Regulated by sympathetic nervous system • Activates sweat glands • Sensible or insensible-500-600 cc/day • Directly related to stimulation of sweat glands • Respiration • Insensible • Increases with rate and depth of respirations, oxygen delivery • About 400 cc/day • Gastrointestinal tract • In stool • Average about 100-200 • GI disorders may increase or decrease it.
Acid-Base Balance • pH measures amount of Hydrogen ion concentration • Greater the concentration, lower the pH • 7 is neutral; <7 acidic; >7 basic or alkaline • Needed to maintain cell membrane integrity and speed of cellular enzymatic actions • Normal range – 7.35-7.45 • Regulated by buffers
Physiological Regulation • Lungs and Kidneys • Lungs adapt fast • Try to correct pH before biological buffers kick in • Hydrogen and carbon dioxide levels provide stimulus for respirations • Lungs alter depth and rate according to hydrogen concentration • With metabolic acidosis, respirations increase to exhale more carbon dioxide • Metabolic alkalosis, lungs retain carbon dioxide by decreasing respiraitons • Kidneys take from a few hours to several days • Reabsorb bicarbonate in case of acid excess; excrete it in cases of acid deficit
Common Disturbances Electrolyte Balance • Sodium • Hypernatremia (Na > 145, sp gravity < 1.010) • Caused by excess water loss or overall sodium excess • Excess salt intake, hypertonic solutions, excess aldosterone, diabetes insipidus, increased s water loss, water deprivation • S&S: thirst, dry, flushed skin, dry, stick tongue and mucous membranes • Hyponatremia (Na < 135, sp gravity > 1.030) • Occurs with net loss of sodium or net water excess • Kidney disease with salt wasting, adrenal insufficiency, GI losses, increased sweating, diuretics, SIADH • S&S: personality change, postural hypotension, postural dizziness, abd cramping, n&v, diarrhea, tachycardia, convulsions and coma
Common Disturbances Electrolyte Balance • Potassium • Hyperkalemia (K > 5.3; EKG irregularities-bradycardia, heart block, wide QRS pattern-cardiac arrest) • Primary cause: renal failure; major symptom: cardiac irregularity • Fluid volume deficit, massive cell damage, excess K+ given, adrenal insufficiency, acidosis, rapid infusion of stored blood, potassium-sparing diuretics • S&S: dysrhythmias, paresthesia • Hypokalemia (K < 3.5; EKG irregularities-ventricular) • Most common electrolyte imbalance; affects cardiac conduction and function. Most common cause: potassium wasting diuretics • Diarrhea, vomiting, alkalosis, excess aldosterone secretion, polyruia, extreme sweating, insulin to treat diabetic ketoacidosis • S&S: weakness, ventricular dysrhythmias, irregular pulse
Common Disturbances Electrolyte Balance • Calcium • Hypercalcemia (Ca > 5; x-rays show calcium loss, cardiac irregularities) • Frequently symptom of underlying disease with excess bond resorption and release of calcium • Hyperparathyroidism, malignant neoplastic disease, Paget’s disease, Osteoporosis, prolonged immobization, acidosis • S&S: anorexia, nausea and vomiting, weakness, kidney stones • Hypocalcemia (Ca < 4.0, EKG abnormalities) • Seen in severe illness • Rapid blood transfusion with citrate, hypoalbuminemia, hypoparathyroidism, Vitamin D deficiency, Pancreatitis, Alkalosis • S&S: numbness and tingling, hyperactive reflexes, positive Trousseau’s sign (wrist), positive Chvostek’s sign (cheek), tetany, muscle cramps, pathological fracture
Common Disturbances Electrolyte Balance • Chloride • Usually seen with acid-base imbalance • Hyperchloremia (Na >145, Bicarb <22) • Serum bicarbonate values fall or sodium rises • Hypochloremia (pH > 7.45) • Excess vomiting or N/G drainage; loop of thiazide diuretics because of sodium excretion • Leads to metabolic alkalosis due to reabsorption of bicarbonate to maintain electrical neutrality
Acid Base Balance • Arterial blood gas is best measure • pH • Measures hydrogen ion concentration • 7.35-7.45 • PaCO2 • Measures carbon dioxide (pulmonary ventilation) • 35-45 < hyperventilation; > hypoventilation • PaO2 • Oxygen in arterial blood • 80-100 • Oxygen Saturation • How much hemoglobin is carrying oxygen • 95-99% • Base Excess • How much blood buffer is present • High – alkalosis Caused from: Antacids, rapid blood transfusion, IV bicarb • Low – acidosis Caused from: Diarrhea • Bicarbonate • Major renal component of acid-base balance • Excreted and reproduced by kidneys • 22-26; 20 times the level of carbonic acid : low is metabolic acidosis, high alkalosis
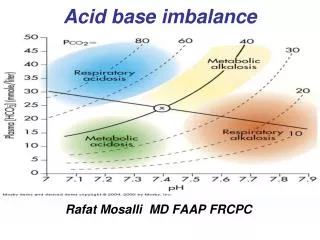
Common Disturbances in Acid-Base Balance • Respiratory acidosis (pH <7.35; CO2> 45;) • Increased carbon dioxide, excess carbonic acid, increased hydrogen ion concentration • Causes: HYPOVENTILIATION • Atelectasis, pneumonia, cystic fibrosis, respiratory failure, airway obstruction, chest wall injury, overdose, paralysis of respiratory muscles, head injury, obesity • S&S: neurological changes and respiratory depression • Confusion, dizziness, lethargy, headache, ventricular dysrhythmias, warm flushed skin, muscular twitching
Common Disturbances in Acid-Base Balance • Respiratory alkalosis (pH > 7.45; CO2 < 35;) • Decreased carbon dioxide, decreased hydrogen ions • Causes: hyperventilation • asthma, pneumonia, inappropriate ventilator settings, anxiety, hypermetabolic state, CNS disorder, salicylate overdose • S&S: dizziness, confusion, dysrhythmia, tachypnea, numbness and tingling, convulsions, coma
Common Disturbances in Acid-Base Balance • Metabolic acidosis (pH < 7>35; Bicarb < 22) • Increased acid (hydrogen ions, decreased sodium bicarbonate • High Anion Gap (Sodium minus Chlorine + Bicarb) • Causes: starvation, diabetic ketoacidosis, renal failure, lactic acidosis, drug use (paraldehyde, aspirin) • S&S: tachypnea with deep respirations, headache, lethargy, anorexia, abdominal cramps
Common Disturbances in Acid-Base Balance • Metabolic alkalosis • Loss of acid (hydrogen ions) or increase bicarbonate • Most common cause: vomiting and gastric secretions • Hypokalemia, hypercalcemia, excess aldosterone, use of drugs (steroids, bicarb, diuretics) • S&S: numbness and tingling, tetany, muscle cramps
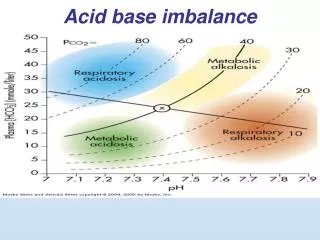
Assessing Blood Gases • 1st look at pH • Over 7.45 Alkalosis • Below 7.35 Acidosis • 2nd check CO2 • Should move in opposite direction as pH • if abnormal, respiratory cause • if normal, metabolic • 3rd evaluate bicarbonate • Should move in same direction as pH • If so, metabolic cause • if not, respiratory cause • 4th both CO2 and bicarbonate abnormal? • Which more closely corresponds to pH and deviates more from normal? • Shows likely cause, other is trying to compensate
Hypercalcemia • Most common causes (90% of cases): • Malignancy associated hypercalcemia • Tumor production of PTH-related protein is the commonest paraneoplastic endocrine syndrome, accounting for most cases of hypocalcemia in inpatients • Primary hyperparathyroidism • Most common cause in ambulatory patients
Hypercalcemia - symptoms • Symptoms • (usually occur if serum calcium is > 12mg/dl and tend to be more severe if hypercalcemia develops acutely) • Constipation • Polyuria • Heart • Ventricular extrasystoles and idioventricular rhythm • Neurologic symptoms • Stupor, coma, azotemia in severe cases
Hypercalcemia - TX • Treatment • Ultimate goal – locate primary disease process & control • Treatment of hypercalcemia of malignancy • Bisphosponates – effective in 95% of cases • Emergency tx of choice • Saline & furosemide (prevent volume overload and enhances Ca2+ excretion)
Hypocalcemia • Often mistaken as a neurological disorder • Most common cause • renal failure • Other causes: • Malabsorption • Vitamin D deficit • Alcoholism • Diuretic therapy • Endocrine disease
Hypocalcemia - Symptoms • Hypocalcemia increase excitation of nerve and muscle cells, primarily affecting the neuromuscular and cardiovascular systems
Hypocalcemia - Symptoms • Symptoms: • Muscle cramps and tetany • Laryngospasm w/stridor • Convulsions • Paresthesias of lips & extremities • Abdominal pain
Hypocalcemia - Symptoms • Chvostek’s & Trousseau’s signs are usually readily elicited • Chvostek’s sign • Contraction of the facial muscle in response to tapping the facial nerve anterior to the ear • Trousseau’s sign • Carpal spasm occurring after occlusion of the brachial artery with a bp cuff for 3 minutes
Hypocalcemia - Labs • ECG: • Prolonged QT interval • Serum calcium concentration: • < 9mg/dl • Serum magnesium • usually low • Serum phosphate level • usually elevated in hypoparathyroidism or end-stage renal failure • Suppressed in early stage renal failure or vitamin D deficiency
Hypocalcemia - Tx • Severe, symptomatic hypocalcemia • 10-15 milligrams of calcium per kilogram of body weight, or 6-8 10-ml vials of 10% calcium gluconate (558-744mg of calcium) added to 1 liter of D5W and infused over 4-6hrs. Adjust infusion rate to maintain serum calcium level at 7-8.5mg/dL • In presence of tetany, arrhythmias or seizures • Calcium gluconate 10% (10-20 ml) IV over 10-15min
Hypocalcemia - Tx • Asymptomatic Hypocalcemia • Oral calcium 1-2g and vitamin D preparations are used
Hyperkalemia • Many cases associated with acidosis • Pseudohyperkalemia – result of lysis of red cells releasing potassium into the serum
Hyperkalemia • Associated With: • HIV • diabetic ketoacidosis • Medications • Surgical Med - Aminocaproic acid • Ace Inhibitors • Trimethoprim • Immunosuppressive medications
Hyperkalemia • Findings • Muscle weakness • Abdominal distention • Diarrhea • Rare finding – flaccid paralysis
Hyperkalemia • Heart rate may be slow, V-Fib & cardiac arrest may occur • ECG changes include: • Peaked T waves, widening of QRS, biphasic QRS-T complexes • Note:nearly 50% of cases with serum levels 6.5meq/L or greater will not exhibit ECG changes
Hyperkalemia - TX • Confirm elevated level of serum potassium (measure in plasma rather than serum) • Tx consists of witholding potassium and giving cation exchange resins by mouth or enema • Sodium polystyrene sulfonate 40-80g/d
Hyperkalemia – Emergent TX • Indicated if cardiac toxicity or muscular paralysis present or if hyperkalemia severe > 6.5-7 meq/L • Calcium gluconate 10% 5-30ml IV • NaHCO3 44-88 meq (1-2 ampules) IV • Insulin 5-10 units, IV plus glucose 50% 25g,1 ampule, IV • Nebulized albuterol 10-20mg in 4 ml normal saline inhaled over 10 min
Hyperkalemia – Nonemergent Tx • Loop diuretic (Furosemide) 40-160mg IV or orally w or w/o NaHCO3, 0.5-3 meq/kg daily • Sodium polystyrene sulfonate (Kayexalate) oral: 15-30g in 20% sorbitol (50-100mL) rectal: 50g in 20% sorbitol • Hemodialysis • Peritoneal Dialysis
Hypokalemia • Severe hypokalemia may induce dangerous arrhythmias or rhabdomyolysis • Self limited hypokalemia occurs in 50-60% of trauma patients (possibly related to enhanced release of epinephrine) • Hypokalemia in the presence of acidosis suggests profound potassium depletion and requires urgent tx
Hypokalemia - Signs • Common findings • Muscular weakness • Muscle cramps • Fatigue • Constipation or ileus
Hypokalemia - Labs • ECG • Decreased amplitude • T wave broadening • Prominent U waves • PVCs • Depressed ST segment
Hypokalemia – Causes Several Causes of Hypokalemia • Decreased potassium intake • Potassium shift into the cell • Renal potassium loss • Primary hyperaldosteronism • Renovascular HTN • Cushing’s Syndrome • Bartter’s Syndrome • Metabolic acidosis • Extrarenal potassium loss • Vomiting, diarrhea, laxative abuse, • Zollinger-Ellison syndrome
Hypokalemia- Tx • Mild to moderate deficiency • Oral potassium • 20 meq/L to prevent hypokalemia, • 40-100 meq/L over a period of days to weeks to treat hypokalemia and fully replete potassium stores
Hypokalemia - TX • Moderate to severe • Peripheral IV should not exceed 40meq/L at rates up to 40 meq/L/h • Continuous ECG monitoring indicated • Check serum potassium q 3-6 hours • Correct magnesium deficiency