Download
1 / 17
210 likes | 750 Views
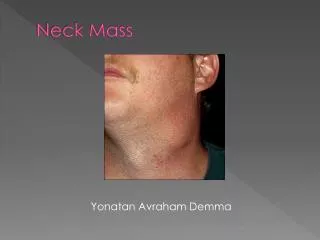
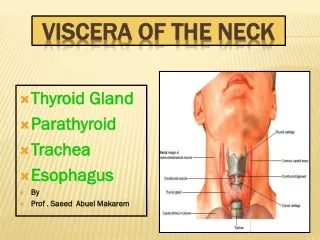
Evaluation of the Neck Mass. Michael Hong, MD. University of Florida Department of Surgery. Neck Mass - History. Age Rate of growth: Days / Months / Years Days – think infectious Months – think cancer Years – think congenital Fever / cough / sore throat

E N D
Evaluation of the Neck Mass Michael Hong, MD University of Florida Department of Surgery
Neck Mass - History • Age • Rate of growth: Days / Months / Years • Days – think infectious • Months – think cancer • Years – think congenital • Fever / cough / sore throat • Recent travel, bites, animal exposure • Weight loss / night sweats • Fatigue / cold intolerance, wt gain • Nervousness, sweating, heat intolerance, exopthalmos, palpitations • Smoking / alcohol use / hx radiation • Trauma • Family history
Location of neck mass Lateral neck, central neck, supraclavicular, cervical Size Soft / Hard Mobile / fixed Painful / Painless Lymphadenopathy Physical Exam
Differential Diagnosis • Congenital • Lateral neck • Branchial cyst, sinus, fistula near SCM • Slow, soft, painless • Workup: FNA + biopsy • Tx: Excision • Medial neck • Thyroglossal duct cyst • thyroid gland usually travels from the base of the tongue to the neck. • Moves when swallowing • Workup: TFT, thyroid scan • Tx: Excision + removal of central hyoidbone (Sistrunk procedure) • Ectopic thymus, parathyroid, thyroid • Mandible – pharyngeal cyst • Congenital torticollis – soft tissue swelling • birth trauma, intrauterine positioning
Differential Diagnosis • Infectious • Abscess – staph / strep / polymicrobial • Tx: abx +/- drainage • TB – single large node, usu. painless, cervical • Workup: PPD, rule out HIV • Tx: Anti-TB meds • Cat scratch fever – Bartonellahenselae • Single enlarged node • Weeks to months after exposure • Self limited • Mono – get EBV titer • p/w cervical adenopathy
Hyperthyroid / hypothyroid • Goiter – enlargement of thyroid gland • Iodine deficiency, Grave’s disease, Toxic Multinodular Goiter, acute/subacute/chronic thyroiditis
Tumors • Benign • Tx: surgical excision • Examples: • Lipoma • Hemangioma • Neuroma • Fibroma • Carotid body tumor
Tumors • Malignant • Primary • Thyroid cancer • Salivary gland cancer (near ear or angle of mandible) • Lymphoma (lateral neck, rubbery and mobile) • Sarcoma • Secondary • metastases
Location of metastases • Supraclavicular – check for chest malignancy • Virchow’s node – left supraclavicular area
Thyroid masses • Benign thyroid nodule – palpable • Follicular adenoma • Colloid nodule • Benign cyst • Solitary toxic adenoma (dec TSH, inc T3 & T4) • Tx: radioactive iodine or unilateral lobectomy
Thyroid cancer • Thyroid cancer • Papillary – young, prior radiation, good prognosis • Good 131 I uptake • Lobectomy and isthectomy • Total Thyroidectomy if diffuse/bilateral disease • Follicular adenoma – cannot dx w/FNA • Good 131 I uptake • Mets to bone • Males 3:1 • Lobectomy and isthectomy • Total Thyroidectomy if large/diffuse
Thyroid cancer cont. • Thyroid cancer • Medullary Carcinoma • Associated with MEN II • Secretes calcitonin • Poor 131 I uptake • Poor prognosis • Tx: total thyroidectomy and median lymph node dissection. • modified neck dissection if lateral cervical nodes are positive. • Hurthle cell – cannot dx with FNA • Adenoma - Lobectomy and Isthmectomy • Carcinoma - Total Thyroidectomy and modified radical neck dissection if lat nodes are positive.
Thyroid cancer cont • Thyroid cancer • Anaplastic • Poor 131I uptake • Giant cells / spindle cells on histology • Bad prognosis • Total thyroidectomy if resectable (usu. Not)
Parathyroid • Primary hyperparathyroidism • Adenoma (85%) • MEN I, MEN IIa • High PTH, high Ca • Tx: excision, confirm with intraoperative PTH • Hyperplasia • MEN I, MEN IIa • Tx: remove all but one parathyroid, intraoperative PTH • Carcinoma • Palpable mass • High PTH, high Ca • Tx: resection of gland, ipsilateral thyroid lobectomy, and ipsilateral lymph node resection.
General Workup Approach • Rule out infectious • EBV, heterophil titer (mono), HIV, PPD • Abx trial • Check thyroid / parathyroid • TSH/T3/T4, PTH/Ca, calcitonin • Fine needle aspiration • Imaging • Ultrasound: cystic vs. solid • Radionucleotide thyroid scan • Cold – 25% malignant • Hot – 5% malignant • CXR, CT (look for primary), MRI (upper neck, skull base)
Fine Needle Aspiration • Fine needle – 25 gauge • Multiple aspirations • Used with US • 5% false negative rate • Cannot distinguish benign/malignant follicular thyroid tumors or Hurthle cell tumors • Good for cysticsvs inflammatory, papillary, medullary, anaplastic cancers
Endoscopy • direct laryngoscopy, esophagogastroscopy or bronchoschopy • FNAB positive with no primary on repeat exam • FNAB equivocal/negative in high risk patient • Biopsy on obvious abnormality • Guided biopsy based on lymphatic drainage