Download
1 / 14
140 likes | 405 Views
Supporting GP Consortia. NHS EAST MIDLANDS. Workshop materials. November 2010. CONFIDENTIAL AND PROPRIETARY Any use of this material without specific permission of McKinsey & Company is strictly prohibited. Four key issues to solve to get GP commissioning right. Focus today.

E N D
Supporting GP Consortia NHS EAST MIDLANDS Workshop materials November 2010 CONFIDENTIAL AND PROPRIETARY Any use of this material without specific permission of McKinsey & Company is strictly prohibited
Four key issues to solve to get GP commissioning right Focus today • Control: Ownership over delegated budgets both for improved services and managing performance • Management cost: Balance need for local relationships and scale • Risk: Pool and cap within NHS • Performance: Manage the money and outcomes at practice and cluster level from day one
Contents • An approach to management cost • An approach to financial risk
7 GP consortia commissioning costs are projected to be about £28 per head after management cost reduction £ per head Management costs Non-management costs 37 28 17 17 All spend1 Non-GP consortia commissioning costs2 Initial consortia commissioning costs 45% mgt costs reduction Final consortia commissioning costs 1 All commissioning spend, i.e., excluding all provision spend and all training spend 2 Commissioning Board, Local Authorities Note: If GP management costs allowance is calculated using management costs definition, the following commissioning costs would count as “non-management” and be excluded: pay costs for non-managers and for managers paid below the salary threshold (~£30k); non-pay costs of GP commissioning, including relevant proportion of shared services, clinical governance
Current NHS commissioning costs are already at the lower end of international health systems WORK IN PROGRESS Operating costs as a % of total health costs, 2009 # managers per 250k patients that this funds1 Mexico New Zealand United States France Germany Netherlands Belgium Slovak Republic Slovenia Canada Austria Czech Republic Spain Korea Current NHS Estonia Finland Iceland Poland Sweden Hungary Norway Italy 1 250k chosen as representative of small PCT. Calculation assumes average all-in pay costs of $75k / £50k for managers SOURCE: For non-UK countries: OECD 2010 HC7 – expenditure on health administration & insurance; CIA world factbook (population); UK data not in OECD analysis, so for current NHS, £64 per capita mgt spend used: team analysis
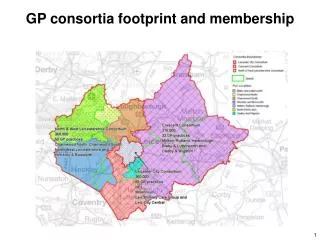
0 • A minimum size is required for a budget that breaks even on fixed costs (approx. 150,000 lives) • Larger sizes then allow for more budget that can be spent on managers and other resources etc. • How many managers will you need? What roles will they play? E.g. • Accountable officer • Finance director • Medical director • Strategy • Operations (contracts) • etc. Larger consortia can invest more in commissioning staff and resources £20 per head A consortium covering 500,000 lives could fund up to ~120 posts 14 13 A consortium covering 250,000 lives could fund up to ~50 posts 12 11 10 9 A consortium covering 50,000 lives could struggle to cover its fixed costs 8 7 Management allowance (£m) 6 5 4 3 £1.6m fixed costs 2 1 0 Population Note: assumes fixed Board costs of £1m, fixed clinical staff costs of £0.6m, and all-in staff costs of £70k per person SOURCE: McKinsey analysis
Suggested questions to discuss 1 Is this sufficiently clear? What are the tradeoffs of a multi-tier arrangement? If you choose to pursue it, what happens at which level? 2 3 What information do you need to make decisions on tradeoffs?
Contents • An approach to management cost • An approach to financial risk
Management risk Variation driven by differences in medical prctice Consortia can directly control via continuous performance management Supply risk Variation driven by differences in provider structure e.g. Hospital density There are four major sources of financial risk... Source of risk Description Implications Consortia may mitigate by being larger, if they cover areas with different demand; DH can reduce via allocation formula Demand risk Variation due to differences in medical demand in the consortium catchment area Consortia may mitigate by being larger in size, if they cover areas with different provider structure Intrinsic risk Variaiton not driven by any distinguishable factor e.g. Random statistical variation Consortia can mitigate by being larger in size SOURCE: McK Medical Risk Group
0 Example: GP Practice A, with 10,000 patients and 4 GPs, would have £2m deficit: that’s £0.5m deficit/GP or £200 deficit/patient …and they will cause deficits in some consortia Surplus Deficit Estimated surplus/deficit for individual GP Practices (2007/08) GP practices Percent • Estimated surplus/deficit at GP Practice level is based on ‘fair share’ of PCT budgets (needs weighted population), and share of commissioning spend • Practices are much more susceptible to variations in spend due to their small size, and so have very wide range of performance (surplus/deficits up to +/-30% of budget) • Total deficits are £3.1bn Example: GP Practice A Sum of deficits: £3.1bn - - - - - - 60 50 40 30 20 10 0 10 20 30 40 Surplus/deficit Percent SOURCE: DH PBC toolkit 2010/11; DH Exposition Books 2007/08
I Use the right allocation formula Increase scale appropriately Reinsure Ensure operational excellence There are four levers that will be used to manage the risk What this means • Government must set allocation formula to match underlying needs of population as closely as possible • Never 100% matched to underlying needs, but can be tweaked • Sets context for GPCC operations • Financial risk falls as consortium size increases • However, it can be tougher to ensure strong mutual accountability in large organisations • Consortia could pool together a contingency in case of problems • Consortia can cut costs, and thus reduce risk of failure, by ensuring operational excellence • This should be main day-to-day focus of commissioners SOURCE: McK Medical Risk Group
Financial risk falls as consortium size increases Example: Consortium A of 10,000 lives would have a deficit every 1 in 3 years Probability of being in deficit by 1% of budget or more Example: Consortium B of 300,000 lives would have a deficit every 1 in 20 years 1,000 3,000 10,000 30,000 100,000 300,000 1M Size of consortiumPopulation SOURCE: McKinsey Medical Risk Group, Monte-Carlo-Simulation based on actual 2008 data of German payor
0 Reinsurance could significantly reduce risk, but at a material cost Example: NHS reinsurance pool for high cost patients set at threshold of 30x average costs Consortia with deficits > 1% of income Percent • Example: if consortia covered 30,000 lives, the fraction who would have deficit >1% would be: • 35% if consortia retained all the risk • 21% if consortia retained 80% of risk • 7% if consortia retained 60% of risk • 2.4% if consortia retained 40% of risk • 0.4% if consortia retained 20% of risk • 0% if consortia retained no risk % of risk retained by GPs [premium as % of income] 100% [0,0%] 80% [0,9%] 60% [1,8%] 40% [2,6%] 20% [3,5%] 0% [4,4%] 1,000 3,000 10,000 30,000 100,000 300,000 1 Mio Size of consortiumNumber of lives covered SOURCE: McKinsey Medical Risk Group, Monte-Carlo-Simulation based on actual 2008 data of German payor
Suggested questions to discuss 1 Is this sufficiently clear? What would be the consequences of a risk coming to fruition, e.g., a deficit occurring? 2 Can you pool together to reduce risk? What would that mean in practice? 3