Download
1 / 41
420 likes | 694 Views
Eating Disorders Among School Age Children. Prepared by: Alaa orsan ali. Presentation outline:. 1- introduction . 2- anorexia nervosa. Definition Characteristics Nursing care plan 3- bulimia nervosa Definition Characteristics Nursing care plan. Presentation outline:. 4-obesity

E N D
Eating Disorders Among School Age Children Prepared by: Alaa orsan ali
Presentation outline: 1-introduction. 2-anorexia nervosa. Definition Characteristics Nursing care plan 3- bulimia nervosa Definition Characteristics Nursing care plan
Presentation outline: 4-obesity Definition Characteristics Nursing care plan 5-eating disorders and community health nursing 6-Article 7-sammary 9-conclusion
Objectives: By the end of this seminar the student will be able to: 1-Define each type of eating disorders. 2 Be familiar with the characteristics of each type 3-Be familiar with nursing care plan for each type 4-value the role of community health nursing in managing eating disorders among school age.
Introduction -Eating behavior is now known to reflect an interaction between an organism’s physiological state and environmental conditions. -Society and culture have a great deal of influence on eating behaviors
introduction EPIDEMIOLOGICAL FACTORS: The incidence of anorexia nervosa has increased in the past 30 years both in the United States and in Western Europe (Halmi, 2008). Anorexia nervosa occurs predominantly in females 12 to 30 years of age. Fewer than 10 percent of the cases are males (American Psychiatric Association [APA], 2000). Bulimia nervosa is more prevalent than anorexia nervosa, with estimates up to 4 percent of young women (Andreasen & Black, 2006).
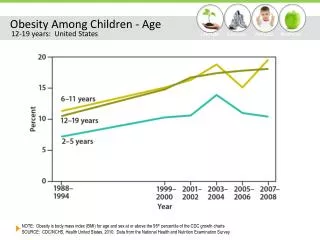
Introduction Obesity: The prevalence of obesity is greater among the lower socioeconomic group (Halmi, 2008), and there is an inverse relationship between obesity and level of education (CDC, 2008).
Anorexia nervosa Anorexia nervosais eating disorder characterized by a morbid fear of obesity and prolonged loss of appetite. Symptoms include: 1-gross distortion of body image (individual perception of being fat when he or she is obviously underweight) 2-refusal to eat.
Symptoms of anorexia nervosa 3-Weight loss is usually accomplished by reduction in food intake and often extensive exercising. 4-Self-induced vomiting 5-abuse of laxatives or diuretics also may occur. 6- Feelings of depression and anxiety
Bulimia nervosa Bulimia nervosa is an episodic, uncontrolled, compulsive, rapid ingestion of large quantities of food over a short period of time (binging), followed by Excessive vomiting and laxative or diuretic abuse. Excessive, insatiable appetite
Symptoms: 1-Excessive vomiting 2-laxative or diuretic abuse 3-lead to problems with dehydration and electrolyte imbalance. 4-Gastric acid in the vomitus also contributes to the erosion of tooth enamel.
Symptoms: 5-tears in the gastric or esophageal mucosa. 6-mood disorders 7-anxiety disorders
Obesity -It is a factor in binge-eating disorder (BED) because the individual binges on large amounts of food (as in bulimia nervosa) but does not engage in behaviors to rid the body of the excess calories. -The following formula is used to determine extent of obesity in an individual: Body mass index =Weight (kg)/Height (m)2 -The BMI range for normal weight is 20 to 24.9 -overweight is defined as a BMI of 25 to 29.9 -obesity is defined as a BMI of 30 or greater.
Obesity who are obese often present with: 1-hyperlipidemia 2-elevated triglyceride and cholesterol levels 3-hyperglycemia 4-risk for developing diabetes mellitus. 5-Osteoarthritis may be evident because of trauma to weight-bearing joints. 6-Workload on the heart and lungs is increased 7-symptoms of angina or respiratory insufficiency (National Heart, Lung,and Blood Institute, 2009).
Care Plan for Client With Eating Disorders: Anorexia Nervosa and Bulimia Nervosa NURSING DIAGNOSES: 1- IMBALANCED NUTRITION: LESS THAN BODY REQUIREMENTS; DEFICIENT FLUID VOLUME (RISK FOR OR ACTUAL) RELATED TO: Refusal to eat/drink; self-induced vomiting; abuse of laxatives/diuretics. EVIDENCED BY: Loss of weight; poor muscle tone and skin turgor; bradycardia; hypotension; cardiac arrhythmias; pale, dry mucous membranes
1-IMBALANCED NUTRITION Short-Term Goals Client will drink 125 mL of fluid each hour during waking hours. Client will gain x pounds per week (amount to be established by client, nurse, and dietitian). Long-Term Goal By time of discharge from treatment, client will exhibit no signs or symptoms of malnutrition or dehydration.
Nursing Interventions and rationale 1. determine number of calories required to provide adequate nutrition and realistic weight gain with the help of the Dietitian. Rationale: Adequate calories are required to allow a weight gain of 2–3 pounds per week. 2. Explain to the client that privileges and restrictions will be based on compliance with treatment and direct weight gain. Do not focus on food and eating. Rationale: The real issues have little to do with food or eating patterns. Focus on the control issues that have precipitated these behaviors.
Nursing Interventions and rationale 3. Weigh client daily, immediately upon arising and following first voiding. Always use same scale, if possible. Keep strict record of intake and output. Assess skin turgor and integrity regularly. Assess moistness and color of oral mucous membranes. Rationale: These assessments are important measurements of nutritional status and provide guidelines for treatment.
Nursing Interventions and rationale 4. If weight loss occurs, use restrictions.Client must understand that if nutritional status deteriorates, tube feedings will be initiated. This is implemented in a matter-of-fact, nonpunitive way. Rationale: Restrictions and limits must be established and carried out consistently to avoid power struggles, to encourage client compliance with therapy, and to ensure client safety
Nursing Interventions and rationale 5. Encourage the client to explore and identify the true feelings and fears that contribute to maladaptive eating behaviors. Rationale:Emotional issues must be resolved if these maladaptive responses are to be eliminated.
Care Plan for Client With Eating Disorders: Anorexia Nervosa and Bulimia Nervosa NURSING DIAGNOSIS: 2-DISTURBED BODY IMAGE/LOW SELF-ESTEEM RELATED TO: Retarded ego development and dysfunctional family system EVIDENCED BY: Distorted body image, difficulty accepting positive reinforcement, depressed mood and self-deprecating thoughts
Care Plan for the Client With an Eating Disorder: Obesity NURSING DIAGNOSIS: 1-IMBALANCED NUTRITION: MORE THAN BODY REQUIREMENTS RELATED TO: Compulsive overeating EVIDENCED BY: Weight of more than 20 percent over expected body weight for age and height; BMI ≥ 30
1-IMBALANCED NUTRITION Short-Term Goal: Client will verbalize understanding of what must be done to lose weight. Long-Term Goal: Client will demonstrate a change in eating patterns that results in a steady weight loss.
Nursing Interventions and rationale: 1. Discuss feelings and emotions associated with eating. Rationale: This helps to identify when the client is eating to satisfy an emotional need rather than physiological one.
Nursing Interventions and rationale: 2.With input from the client, formulate an eating plan that includes food from the required food groups with emphasis on low-fat intake. It is helpful to keep the plan as similar to client’s usual eating pattern as possible Rationale:Diet must eliminate calories while maintaining adequate nutrition Client is more likely to stay on the eating plan if he or she is able to participate in its creation and it deviates as little as possible from usual types of foods.
Nursing Interventions and rationale: 3. Identify realistic increment goals for weekly weight loss. Rationale:Reasonable weight loss (1–2 lb per week) results in more lasting effects. Excessive, rapid weight loss may result in fatigue and irritability and ultimately lead to failure in meeting goals for weight loss. Motivation is more easily sustained by meeting “stair-step” goals. 4.Plan progressive exercise program tailored to individual goals and choice Rationale: Exercise may enhance weight loss by burning calories and reducing appetite, increasing energy, toning muscles, and enhancing sense of well-being and accomplishment. Walking is an excellent choice for overweight individuals.
Care Plan for the Client With an Eating Disorder: Obesity NURSING DIAGNOSIS: 2- DISTURBED BODY IMAGE/LOW SELF ESTEEM RELATED TO: Dissatisfaction with appearance EVIDENCED BY: Verbalization of negative feelings about the way he or she looks and desire to lose weight
Topics for Client/Family Education Related to Eating Disorders Nature of the Illness 1. Symptoms of anorexia nervosa 2. Symptoms of bulimia nervosa 3. What constitutes obesity 4. Causes of eating disorders 5. Effects of the illness or condition on the body
Topics for Client/Family Education Related to Eating Disorders Management of the Illness: 1. Principles of nutrition (foods for maintenance of wellness) 2. Ways client may feel in control of life (aside from eating) 3. Importance of expressing fears and feelings, rather than holding them inside 4. Alternative coping strategies (to maladaptive eating behaviors)
Topics for Client/Family Education Related to Eating Disorders 5. For the obese client: a. How to plan a reduced-calorie, nutritious diet b. How to read food content labels c. How to establish a realistic weight loss plan d. How to establish a planned program of physical activity
Topics for Client/Family Education Related to Eating Disorders 6. Relaxation techniques 7. Problem-solving skills
Article: Impact of a nurse-directed, coordinated school health program to enhance physical activity behaviors and reduce body mass index among minority children: A parallel-group, randomized control trial.
Article: Background: Underserved children, particularly girls and those in urban communities, do not meet the recommended physical activity guidelines (>60 min of daily physical activity), and this behavior can lead to obesity . The school years are known to be a critical period in the life course for shaping attitudes and behaviors. Objectives: To evaluate the impact of a nurse directed, coordinated, culturally sensitive, school-based, family-centered lifestyle program on activity behaviors and body mass index.
Article: Design, settings and participants: a community-based participatory research approach, through a partnership with a University and 5 community schools. Participants included 251 children ages 8–12 from elementary schools in urban. Methods: a 6-week program which met weekly to provide 45 min of structured physical activity and a 45 min nutrition education class for parents and children . Physical Activity and Nutrition Student Questionnaire measured physical activity behavior, including: daily physical activity, participation in team sports, attending physical education class, and Tv viewing/computer game playing. Anthropometric measures included height, weight, body mass index,
Article: Results: Significant results for students in the intervention, included for boys decreases in TV viewing; and girls increases in daily physical activity, physical education class attendance, and decreases in body mass index z-scores from baseline to the 12 month follow-up. Conclusions: Our study shows the value of utilizing nurses to implement a culturally sensitive, coordinated, intervention to decrease disparities in activity and TV viewing among underserved girls and boys.
summery The incidence of eating disorders has continued to increase over the past 30 years. Individuals with anorexia nervosa, a disorder that is characterized by a morbid fear of obesity and a gross distortion of body image, literally can starve themselves to death. The individual with anorexia nervosa believes he or she is fat even when emaciated. The disorder is commonly accompanied by depression and anxiety. Bulimia nervosa is an eating disorder characterized by the consumption of huge amounts of food, usually in a short period of time, and often in secret. With bulimia nervosa, tension is relieved and pleasure felt during the time of the binge, but is soon followed by feelings of guilt and depression.
Summary: ■ Individuals with bulimia nervosa “purge” themselves of the excessive intake with self-induced vomiting or the misuse of laxatives, diuretics, or enemas. They also are subject to mood and anxiety disorders. ■ Compulsive eating can result in obesity, which is defined by the National Institutes of Health as a body mass index (BMI) of 30. ■ Treatment modalities for eating disorders include behavior modification, individual psychotherapy,family therapy, and psychopharmacology
Conclusion ■ Predisposing factors to eating disorders include genetics, physiological factors, family dynamics, and environmental and lifestyle factors. And as a community health nurse we can control some of these factors by health education of the client and the family.
References: Essentials of Psychiatric Mental Health Nursing Concepts of Care in Evidence-Based Practice. FIFTH EDITION Mary C. Townsend, dsn, pmhcns-bc