Download
1 / 8
80 likes | 215 Views
Implementation of a Hypothermia Treatment Program for Hypoxic Ischemic Encephalopathy- SCVMC NICU Experience.

E N D
Implementation of a Hypothermia Treatment Program for Hypoxic Ischemic Encephalopathy- SCVMC NICU Experience Implementation of this program would not have been possible without extreme dedication of SCVMC NICU staff and families, and support from Santa Clara County First Five and Valley Medical Center Foundation.
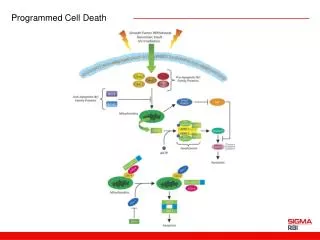
Brain injury evolves over time following hypoxic-ischemic insult Primary cell death Cytotoxic mechanisms Delayed neuronal death - Hypothermia 72 hrs HI 6 hours Days Epo and other intervention + Repair mechanisms
SCVMC Total Body Cooling (TBC) INCLUSION: ≥36wks GA and ≥ 1800gms AND meet both Physiologic and Neurological Criteria EXCLUSION: 1)Lethal Chromosomal or Congenital anomalies, 2) Active bleeding, 3) Severely injured - comfort care Physiological Criteria Neurological Criteria Cord or Baby’s ABG < 1 hour Moderate Encephalopathy 3 of 6 findings below 1. Lethargic 2. Inactive/decreased activity 3. Distal flexion 4. Hypotonia- focal or general 5. Weak suck/incomplete moro 6. Pupil constricted/ Bradycardia/periodic breathing No gas <1hr OR pH 7.01-7.15 and BD 10-15.9 pH ≤7.0 OR BD ≥16 Plus OR A Major Perinatal Event 1. FHR decals, cord prolapse, abruption,uterine rapture, 2. Maternal trauma, hemorrhage 3. Infant CPR in DR AND Apgar ≤ 5 at 10 min or PPV ≥ 10 min Severe Encephalopathy 3 of 6 findings below 1. Stupor/coma 2. No activity 3. Decerebrate 4. Flaccid tone 5. Absent suck/moro 6. Pupils dilated /unreactive, variable HR, apnea Physiological Criteria NeurologicalCriteria AND Active Cooling OR Seizure On Clinical Exam or BrainZ
First infant 47 infant Feb 08 2007 2008 2009 2010 2011 2012 Epo study Skills Lab Hands-on Staff Ed. Completion of Epo study Staff In-service HIE and TBC Nursing P and P Lit. Review Program Set Up Cooling during transport Trial Start Data Submission to VON - NER Bay Area 3rd Cooling Summit Nursing Medical P and P Revised Supper User Skills day Train aEEG “Super Users” Cooling Equipment Changed VON NICQ Encephalopathy collaborative
QI paper – Pediatrics in press • Optimizing Therapeutic Hypothermia for Neonatal Encephalopathy: A Quality Improvement Collaborative Using Potentially Better Practices • ¹Steven L. Olsen, MD, ²Mitchell DeJonge, MD, ³Alex Kline, MD, 4Ellina Liptsen, MD, 5Dongli Song, MD, PhD, ¹Betsi Anderson, RN, BSN, CPHQ, 6Amit Mathur, MBBS, MD
Long-Term Neurodevelopmental Outcomes? Evaluation of Brain Injury and Prognosis?