Download
1 / 46
1.36k likes | 2.97k Views
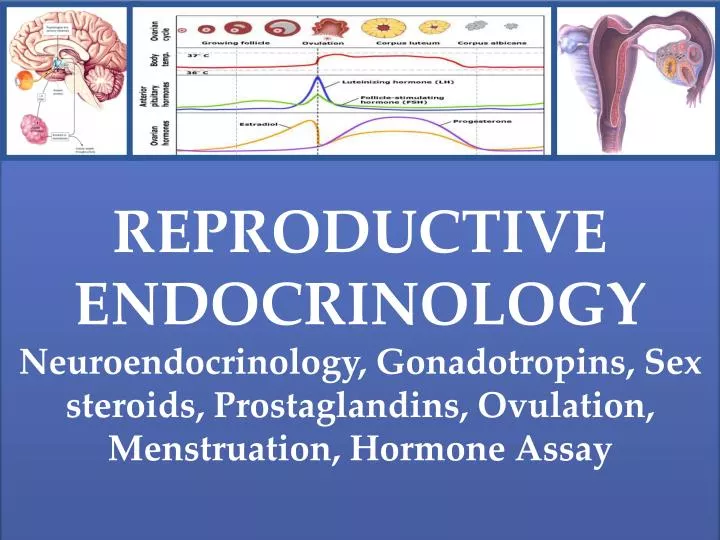
REPRODUCTIVE ENDOCRINOLOGY Neuroendocrinology, Gonadotropins, Sex steroids, Prostaglandins, Ovulation, Menstruation, Hormone Assay. OBJECTIVES. To review the basic anatomic, histologic, and biochemical concepts governing the hypothalamic-pituitary-ovarian (HPO)axis.

E N D
REPRODUCTIVE ENDOCRINOLOGY Neuroendocrinology, Gonadotropins, Sex steroids, Prostaglandins, Ovulation, Menstruation, Hormone Assay Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
OBJECTIVES • To review the basic anatomic, histologic, and biochemical concepts governing the hypothalamic-pituitary-ovarian (HPO)axis. • To discuss the cyclic changes in hypothalamic, pituitary, and ovarian hormones and other growth factors in relation to the menstrual cycle. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology HPO Axis: An overview Failure of GnRH neuronal migration and subsequent establishment of functional connection between brain and hypophyseal portal system results in KALLMANN SYNDROME. HYPOTHALAMUS release of GnRHwhich stimulates release of LH and FSH from the adenohypophysis (ANTERIOR PITUITARY) GnRH neurons originate from progenitor cells in the embryonic olfactory placode where they develop and migrate during ealry fetal life toward the brain. 16 weeks fetal life: functional connections between GnRH neurons and the hypophyseal portal system is established. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Hypothalamic- • Pituitary Transport of GnRH • Via Portal Vessels of the • Superior Hypophyseal Artery ARCUATE NUCLEUS - greatest number of GnRHneurons Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology GnRH: a Decapeptide (10 a.a.) GnRH gene is situated on Chr 8p encoding for a 92 a.a. precursor molecule for GNRH: 1) signal peptide sequence (13 a.a. long) 2) GnRH sequence itself (10 a.a. long) 3) posttranscriptional processing signal (3 a.a. long) 4) GAP/ GnRH associated peptide (56 amino acid peptide) GnRH (short half-life): t 1/2 of 2-4 mins. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology HYPOTHALAMUS: Pulsatile Release of GnRH GnRH pulses: occurs at an hourly interval Rising edge of each GnRH pulse is abrupt, increasing by a factor of 50 within 1 minute. GnRH Pulse Generator Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Mechanisms Responsible for GnRHPulsatility: • The cellular basis and the mechanisms that determine the timing of the increase in multiunit activity resulting in pulsatile GnRH activity are still under study. • There is a growing consensus that pulsatile activity originates from an inherent pace-making activity of theGnRH neuron itself: synchronized action occur through gap junctions between GnRH neuron • Role of Kisspeptin (KISS1), product of KISS1 gene and its receptor (GPR54 or KISS1R) in GnRH regulation - KISS1 neurons directly innervate and stimulate GnRH neurons and is now implicated in mediating sex steroids feedback loops especially during preovulatoryGnRH/LH surge. The presence of the estrogen and the androgen receptorsin KISS1 neurons within the arcuatenucleus modulates the feedback loops. • KISS1 also has been shown to play a role in initiation of puberty. • Mutation or targeted deletions in KISS1 or its receptor = HYPOGONADOTROPIC HYPOGONADISM Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Modulatory influences on GnRH release: • Foremost modulatory influence on frequency and amplitude of GnRH pulses is the ovarian steroid hormones. • Estradiol decrease GnRH • pulse amplitude. • Progesterone decreases GnRHpulse frequency. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Modulatory influences on GnRH release: These systems may affect the GnRH pulse generator either tonally or conditionally. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Metabolic influences on GnRH release: Growing evidence indicates that complex and extensively integrated physiologic mechanisms connect anactive reproductive axis to the metabolic state (nutritional status). And overall, in regard to the reproductive system, the GnRH pulse generatoractually acts as the link between the environment, the internal milieu, and the reproductive axis. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Anterior Pituitary: also called Adenohypophysis • Is derived from Rathke’s pouch ~ 3rd week of life, in contrast to the posterior pituitary (neurohypophysis) which is a direct extension of the the brain. • Contain gonadotropes – specialized cells that produce gonadotropins. • Gonadotropes contain high affinity GnRH receptors (GnRH-R)found along their cell membranes. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • GnRH-R • Encoded by Chr 4q13.2-13.3 and spans 18.9kb. • Belongs to the family of • G protein-coupled receptors • It contains 7 TM helices connected by 6 alternating IC and EC loops (~NH2 terminus is located on EC side) and lacks a carboxy terminuson IC site in contrast to other protein receptors (i.e LH/ FSH/TSH/ hCG). Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • GnRH-R • Activation of GnRH-R stimulates cellular production of specific membrane-associated DAG* (diacylglycerols) that act as 2nd messenger to activate cellular proteins: • Protein kinase C (PKC) and • Mitogen-activated protein kinase (ERK) • Phosphorylated ERK activatestranscription factors (TF) • Gene transcription of gonadotropin subunits and synthesis of both gonadotropins transient rapid influx of ICCa++ ofEC Ca++ burst of exocytosis activates calmodulin a Calcium-binding protein rapidly release maintaining LH and FSH gonadotropinrelease *DAGamplify the action of Ca++-calmodulin, synergistically enhancing the release of gonadotropins. Calmodulinantagonist = GnRH-stimulated gonadotropin release. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • GnRH-R and Estrogen • Estradiol decreasesGnRH pulse amplitude but its effect on GnRH-R is to increase it. • Increase GnRH-R leads to increase Ca++ response with amplified gonadotropin release per GnRH pulse • Thus GnRHpulses of similar amplitude elicit greater gonadotropin responses during the late follicular phase and luteal phase(whenestradiol levels are highest), but the responses are lower during the early follicular phase (whenestradiol levels are lowest) Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • GnRH Pulse frequency and Gonadotropin release • GnRH pulse frequency besides pulse amplitude regulates gonadotropin subunit gene transcription: • Low GnRH pulse frequency = FSH synthesis • (progesterone effect) • High GnRH pulse frequency = LH synthesis • Changing pulsatile infusion from a high to a low pulse frequency results in an FSH: LH ratio. • This phenomenon may play a role in the changing FSH:LH ratio that occurs during the passage from one menstrual cycle to another FSH:LH LH:FSH =PCOS Clinical example: PCOS = high GnRH pulse frequency, resulting in the pathologic elevation in LH:FSH ratio Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • GnRH-R desensitization • GnRH pulse (pulsatile release) causes rapid release of both FSH and LH (within minutes). • GnRH pulse (continuous release) results in sustained GnRH-R exposure causing reduce response to GnRH stimulation = homologous desensitization/ down-regulation of the receptor. This takes a few days reflecting loss of active cell surface receptors and maintained by a loss of functional Ca++ channels. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology GnRH agonist versus GnRH antagonist: Action on the GnRH-R 1 2 3 4 5 6 7 8 9 10 Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology Anterior Pituitary: Gonadotropins Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Hypothalamic pulsatile release of GnRH • Anterior pituitary pulsatile release of FSH and LH • FSH and LH reaches the Ovary to stimulate cyclic estrogen and progesterone production • Estrogen and progesterone stimulates ovarian folliculogenesis and endometrial menstrual changes Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE OVARIES: OOGENESIS/ GAMETOGENESIS OOGONIA or PRIMORDIAL GERM CELLSdevelop from endoderm then migrate to the genital ridge at 5-6 weeks 600,000 at 2nd month of fetal life 7 million by 6th to 7th month ~ UNDERGO MEIOSIS I forming Primary Oocyte 2-4 Million at birth 300,000 at puberty (90% depleted) 25,000 at age 37 1000 at age 50 Primary oocytes are arrested at Meiosis I – Diplotenestage (germinal vesicular stage) of Prophase at birth Meiosis II is only completed if the oocyte is fertilized Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE • OVARIES: FOLLICULOGENESIS • PRIMORDIAL FOLLICLE – primary oocyte surrounded by a single layer of granulosa cells (GC). • PRIMARY/ PREANTRAL FOLLICLE– primary oocyte surrounded by a multiple layers of granulosa cells (GC); development is not gonadotropin-dependent but influenced by intra-ovarian, nonsteroidal process (occurs during non-ovulatory stages of childhood, pregnancy, oral contraceptive use, and ovulatory cycles). • SECONDARY/ ANTRAL FOLLICLE – under hypothalamic-pituitary control and requires FSH. • MATURE/ PRE-OVULATORY FOLLICLE Arrested in prophase I Arrested in metaphase II Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE • OVARIES: STEROIDOGENESIS • ESTRADIOL • PROGESTERONE • ANDROSTENEDIONE • Also secrete in varying amounts: • Estrone • Pregnenolone • 17-OH progesterone • Testosterone • DHEA • Does not synthesize (d/t lack of appropriate enzymes): • Mineralocorticoid • Glucocorticoid 2- carbon compound 27-carbon steroid 19 carbon atoms 18 carbon atoms 21 carbon atoms Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
STEROIDOGENESIS Steroidogenic acute regular protein Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
STEROIDOGENESIS • Aromatase enzyme • Converts androgens to estrogens (estrone/estradiol) • Complex enzyme comprised of 2 proteins: • 1) P450 arom–member of the cytochrome P450 superfamily of genes, catalyzes reactions for formation of phenolic A ring. • 2) NADPH-cytochrome P450 • reductase– an ubiquitous protein • required for transferring reducing • equivalents from NADPH to any • microsmal form of cytochrome P450 • which it comes in contact. • Found in: ovaries, endometrium, brain, placenta, bone, skin, adipose tissue. Overall, the C18 estrogen produced in different tissue sites is specific and dependent on the nature of the C19 steroid presented to the aromatase enzyme: Clinical application: CYP 19 aromatase gene Mutation = an autosomal recessive disorder leading to aromatase deficiency syndrome. Manifested by accumulation of androgens during pregnancy leading to virilization at birth and hypoestrogenism. AROMATASE INHIBITORS = useful in management of patients with ER + tumors, i.e. Breast CA. In the ovary, the main androgen source is ovarian testosterone and thus the main estrogen product from the ovary is estradiol, whereas In adipose tissue, the main androgen source is circulating androstenedione(produced by the adrenals) and hence the principal estrogen produced is estrone. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Ovarian Steroid: Blood Transport and Metabolism • Transport: 1) SHBG – a β-globulin synthesized by the liver; DHT>Testosterone>E2 affinity • 2) albumin – most biologically important fraction bec. free to diffuse or actively • transported through capillary wall and bind to its receptor • 3) corticosteroid binding protein (CBG or transcortin) – primarily binds adrenal • steroids and progesterone to a lesser degree • Both SHBG & CBG – high affinity but low capacity for steroids vs. Albumin – low affinity • but high capacity hence steroids can readily dissociate and enter target cells. • Metabolism: Liver via oxidation (bile acids) and Kidneys via conjugation to form water soluble products (estradiol-17 glucuronide, estrone sulfate, and pregnanediol-3-glucuronide, the major urinary metabolite of progesterone) Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Ovaries: Prostaglandin action • A subclass of eicosanoids and prostanoids and are general mediators of inflammatory and anaphylactic reactions. • Formed from arachidonic acid which is derived from linoleic acid supplied in the diet. • Formation is inhibitied by NSAIDS type 1 (aspirin and indomethacin) and type 2 (phenylbutazone) and corticosteroids. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Communication within the HPO endocrine axis: • Steroid receptors – found in cytoplasm or nucleus and may undergo shuttling in the absence of hormone(vs cell membrane for peptide hormones); inactive state via multiprotein inhibitory complex (i.e. heat shock proteins,hsp) and activated state that allows binding to hormone responsive element HRE in DNA-binding site. • The Ovarian-hypothalamic-pituitary Feedback Loops: • The Negative Steroid Feedback Loop • The Positive Estradiol Feedback Loop • Ovarian Peptides Feedback Loops Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Communication within the HPO endocrine axis: • The Negative Steroid Feedback Loop • Estradiol-17b • Mainly by controlling the amplitude of each LH pulse, relayed by estrogen-receptive kisspeptin and possibly GABA neurons (hypothalamus). • Inhibitory effect on the pituitary gonadotrope: decrease gonadotropin response to GnRH (involving GnRH-R) • Progesterone • affects mainly the GnRH pulse generator by slowing the frequency of pulses (becomes more pronounced during luteal phase) Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Communication within the HPO endocrine axis: • The Positive Estradiol Feedback Loop • dependent on rapidly rising estradiol levels, in combination with a small but significant progesterone rise, both produced by the mature dominant follicle and responsible for the generation of the preovulatory LH and FSH surge. • serves as the critical signal to the hypothalamic-pituitary axis that the dominant follicle is ready to ovulate. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
Reproductive Endocrinology • Communication within the HPO endocrine axis: • Ovarian Peptides Feedback Loops • nonsteroid ovarian factors exert negative feedback effects on the anterior pituitary • Inhibin A (pk: midluteal) and B (pk: following LH surge) • Preferential inhibition of FSH over LH • through their own negative feedback • loop ~functions at a significantly • slower rate (hours)vs steroid negative • feedback loop (minutes) • Activin A and B • Stimulate FSH release from the pituitary. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE • Ovarian cycle • Follicular phase • Luteal phase • Uterine cycle • Proliferative phase • Secretory phase Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Ovarian cycle • Follicular phase • Luteal phase Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL 3. Rising estrogen levels provide negative feedback on pituitary FSH secretion 4. At the end of the follicular phase (just before ovulation), FSH-induced LH receptors are present on granulosa cells and, with LH stimulation, modulate the secretion of progesterone 2. With the demise of the corpus luteum, FSH levels begin to rise • Ovarian cycle • Follicular phase • Luteal phase 1.At the beginning each menstrual cycle → low levels of gonadal steroids Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL After a sufficient degree of estrogenic stimulation, the pituitary LH surge is triggered, which is the proximate cause of ovulation that occurs 24 to 36 hours later • Ovarian cycle • Follicular phase • Luteal phase Progesterone levels rise precipitously after ovulation and can be used as a presumptive sign that ovulation has occurred Both estrogen and progesterone remain elevated throughout the lifespan of the corpus luteum and then wane with its demise, setting the stage for the next cycle Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Ovarian cycle • Follicular phase 1) Recruitment of a Cohort of Antral Follicles – by FSH 2) Selection of a Dominant Follicle – completed by Day 5 and most probably reflects the competitive advantage of the dominant follicle, characterized by a well-vascularized theca layer better gonadotropin supply to their target receptors, greater local estradiol secretion, which increases the density of gonadotropin receptors and promotes cell multiplication. Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Ovarian cycle • Follicular phase 3) Growth of the Dominant Follicle: The Maturing Secondary or AntralFollicle (Max mean D = 19.5 mm, 18-25 mm; Mean max follicular vol = 3.8mL 3.1-8.2 mL) Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Ovarian cycle • Ovulation During the ovulatory surge: LH levels increase 10-fold over 2 to 3 days FSH levels increase 4-fold. This gonadotropin surge is an absolute requirement for the final maturation of the oocyte and the initiation of the follicular rupture. LH surge initiates germinal vesicle (or nucleus) disruption, and the fully grown oocyte resumes meiosis (meiotic maturation) from the diplotene stage of the first to metaphase II of the second meiotic divisionand completed only during fertilization. Ovulation: 24 hrs after E2 peak 32 hrs after initial LH rise 12-16 hrs after LH pk in serum Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Ovarian cycle • Luteal phase Normal function of the corpus luteumdepends primarily on LH stimulation throughout the luteal phase. Progesterone dominance during the luteal phase affects the hypothalamic thermoregulatory center= small increase in basal body temperature (BBT) Progesterone levels: <1 ng/mL before ovulation vs 10-20 ng/mL at midluteal Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Ovarian cycle • Luteal-Follicular transition phase The end of the luteal phase is characterized by a dramatic decrease in progesterone, estradiol, and inhibin A. This is accompanied by a characteristic divergence in the FSH:LH ratio, now favoring a specific rise in FSH Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Uterine cycle • Proliferative phase The estrogen from the developing follicles acts on the endometrium in the ‘Follicular’ phase, stimulating it to grow or ‘proliferate’. Ovarian Follicular Phase = Endometrial Proliferative Phase Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition. PROLIFERATIVE SECRETORY
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Uterine cycle • Secretory phase The progesterone from the corpus luteum acts on the endometrium in the ‘Luteal’ phase, stimulating the glands to ‘secrete’ and prepare for the implantation of a fertilised egg. The spiral arterioles begin to coil and later become kinked. Ovarian Luteal Phase = Endometrial Secretory Phase Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition. PROLIFERATIVE SECRETORY
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Uterine cycle • Menstruation phase • The life span of the corpus luteum is about 12-14 days • If pregnancy does not occur, it self destructs (‘luteolysis’) • As progesterone production declines, the endometrium loses it support and with the resorption of stromal oedema, the spiral arterioles become more kinked and constricted. • The endometrial tissue becomes necrotic and sheds as menstrual effluent Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition. PROLIFERATIVE SECRETORY
THE MENSTRUAL CYCLE FOLLICULAR LUTEAL • Endometrial Cyclic changes • Decidua functionalis - superficial 2/3 & cycling portion of the endometrium; proliferates and is ultimately shed with each cycle if pregnancy does not occur. • stratum spongiosum- deeply situated intermediate zone • stratum compactum- superficial compact zone the endometrium. • Decidua basalis - deepest region of endometrium. It does not undergo significant monthly proliferation & is the source of endometrial regeneration after each menses CONSTANT VARIABLE Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition. PROLIFERATIVE SECRETORY
THE MENSTRUAL CYCLE Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
theca and granulosa cells transform into the corpus luteum and secrete large amounts of progesterone 10-20 primordial follicles begin to develop in response to FSH and LH levels FSH and LH stimulate theca and granulosa production of estrogen and progesterone if fertilization does not occur, corpus luteum degenerates ... if fertilization does occur, HCG released from the embryo maintains corpus luteum surge of LH induces ovulation In Summary: HPO Axis and Menstrual Cycle HORMONAL REGULATION OF OOGENSIS AND OVULATION OVULATION LUTEAL PHASE FOLLICULAR PHASE Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.
THE MENSTRUAL CYCLE Lentz GM, Lobo RA, Gershenson DM, and Katz VL. Comprehensive Gynecology 2012. 6th Edition.