Download
1 / 49
590 likes | 1k Views
The Pharmacists’ Role in Treating Hypertension. Thomas Owens, MD Saint Francis University CERMUSA. Objectives. Enhance your understanding of hypertension to include cardiovascular risks, management, and goals for individual patients

E N D
The Pharmacists’ Role in Treating Hypertension Thomas Owens, MD Saint Francis University CERMUSA
Objectives • Enhance your understanding of hypertension to include cardiovascular risks, management, and goals for individual patients • Review and discuss the current pharmacotherapy standards of care for hypertension • Describe the pharmacist’s role in counseling patients on hypertensive medications
Hypertension >140/90 mm Hg • United States: 65 million adults • Risk factors include: • Stroke, myocardial infarction, heart failure, peripheral vascular disease, aortic dissection, chronic renal failure • Hypertension price tag: $59.7 billion Wexler & Feldman, 2005
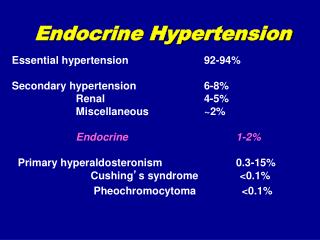
Hypertension • Typical onset • second decade of life • Primary Hypertension • identifiable behaviors • Secondary Hypertension • more discrete Cecil, 2004
African Americans 43% female & 39% male Ratio 1:3 Increase in sodium sensitivity? Caucasians 28% female 29% male Mexican Americans Ratio 1:4 or 1:5 Ethnic Groups DASH Diet Cecil, 2004
Dietary Sodium Intake • Salt Hypothesis? • Strong genetic underpinning ADA, 2005
Metabolic Syndrome • Risk of Hypertension increases with BMI • Obesity accounts for 50% to 60% of new cases of hypertension Cecil, 2004
Sleep Apnea Potential Causes of Hypertension • Expanded plasma volume plus sympathetic over activity • Peripheral vasoconstriction • Renal salt retention • Renal water retention www.sleepconsultants.com, 2007 Cecil, 2004
Blood Pressure Equation Blood Pressure = Cardiac Output x Peripheral Vascular Resistance Most pharmacologic agents lower Some pharmacologic agents lower Some pharmacologic agents lower both Cecil, 2004
Genetics of High BP • Sympathetic up-regulation leads to a cascade of events • Peripheral vascular resistance • Genetic factors • 30% of cases • 2x as likely if parents have hypertension Discoveryedge.mayo.com, 2007; ADA, 2003
Systolic & Diastolic ?? • What is more important? • Depends on age • Live long enough almost all develop systolic hypertension systolic 120 80 diastolic Cecil, 2004
Age Dependant Rise in BP (Whelton & Rocella, 1995)
Framingham Study (age: 50-79) (Khan, Wong, Larson, & Levy, 1999)
Systolic Hypertension • Decreased distensibility of large arteries • Majority of uncontrolled hypertension • Due to focus on diastolic BP Cecil, 2004
Risk of cardiovascular mortality by systolic BP (National High Blood Pressure Education Program Working Group, 1993)
Hypertension Study Results • Hypertension is excess of 140/90 mm Hg • Studies found • Increase risk when above 115 mm Hg systolic or 75 mm Hg diastolic • High normal BP had twice increased risk for cardio disease • More studies are needed to fully understand Cecil, 2004
The Silent Killer • 1/3 of adults do not know they have hypertension • Hypertension: 60% are treated • 45% of treated remain uncontrolled Despite over 75 different antihypertensive agents in 9 different classes! Cecil, 2004
Reclassification of BP Stages • Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC) • New category “pre-hypertension” • Pharmacotherapy not recommended • Lifestyle modification recommended! Cecil, 2004; JNC, 2007
JNC Drug Therapy Recommendations ≥130/80 (w/ heart and kidney disease or diabetes mellitus) recommendation (healthy) JNC, 2007
Modest reduction in BP = big benefits !! • Decrease 5 mm Hg decreases risks • Small changes can have a big difference • Results of studies • Systolic surge 34 mm Hg = 3x increase of stroke • Systolic ≥135 mm Hg = 74% increase of cardio event Cecil, 2004; JNC, 2007
Clinical Presentation • No specific signs or symptoms • Possible symptoms • Occipital headache, dizziness, tinnitus, dimmed vision, palpitations, fatigue • Physical Exam • May reveal evidence Cecil, 2004
Hypertensive Retinopathy Grades of hypertensive retinopathy shown (Forbes, Jackson, 2003)
Electrocardiogram (ECG or EKG) BAD (Antero-Septal MI) GOOD (Normal) physiol.umin.jp/cardiovasc, 2007
Counseling Patients:Proper BP Readings • At least 30 minutes before NO • Caffeine, decongestants, oral contraceptives, alcohol, tobacco • Sit down for at least 5 minutes Cecil, 2004; ADA, 2005
Counseling Patients:Proper Fit of BP Cuff Length of bladder of the cuff at least 80% circumference of arm Bladder of cuff at least 40% circumference of arm Place the center of the bladder over the brachial artery Pump until radial pulse disappears, then continue for additional 30 mm Hg
Help Patients Understand:White Coat Hypertension • Anxiety of going to doctor office raises BP • Recommend self-monitoring • Daytime: >135/85 mm Hg • Nighttime: >120/70 mm Hg • 24 hr: >130/80 mm Hg • Follow patients every 6 months for possible progression to persistent hypertension Cecil, 2004
Closely Monitor Medications with High-Risk Patients Cecil, 2004
Counseling Patients:Treatment JNC, 2005
Counseling Patients:Lifelong Treatment • Objective: reduce BP and metabolic abnormalities • Pharmacotherapy & lifestyle modification • Reduce sodium intake • Weight loss • Exercise • Moderating alcohol • Reduce systolic BP by 21 to 55 mm Hg Cecil, 2004
Counseling Patients:Dietary Changes • Losing only 10 to 12 lbs lowers BP by 10/5 mm Hg • Reduce daily salt • 10 to 6 grams • Teach patients to read food labels • DASH Diet • www.nhlbi.nih.gov/health/public/heart/dash Cecil, 2004
Counseling Patients:Health Behaviors JNC, 2005
Counseling Patients:Helpful Resources www.lotrel.com
Barriers to Successful Health Behavior Modifications • Lack of education • Lack of access to safe places to exercise • Added salt in prepared foods and restaurant meals • Higher cost of foods low in salt Patient self-management is realistic and feasible! Cecil, 2004
Pharmacologic Therapy • Scientific proof lowering BP reduces organ damage • Certain classes of antihypertensive agents exert organoprotective effects • Not all medications equal Cecil, 2004; JNC, 2005
Major Challenges for Science • Identify the key gene-environment interactions • Eliminate the patient and medical provider barriers ADA, 2003
Counseling Patients:Target Blood Pressure • Most patients below 140/90 mm Hg • Patients w/ diabetes or chronic disease 130/80 mm Hg • Help patients self-monitor BP • 1/3 do not know they are hypertensive • Research studies on targeting BP Cecil, 2004
Improve Hypertension Control Rates • Titrating blood pressure medications to achieve target goals • Most patients require 2 or 3 antihypertensive medications • Patient compliance with multi-drug regimens ADA, 2005
Patient Compliance and Quality of Life • Hypertension requires lifelong treatment • Medications can produce side effects • Men often concerned with sexual dysfunction • Patients with controlled BP, rate a significantly higher quality of life Cecil, 2004
Patient Compliance Principles • Titrating medical therapy based on home readings • Long-acting preparations w/ once daily dosing • Low dose combinations of medications from different drug classes • Fixed-dose combinations to reduce overall number of pills JNC, 2005
Drug Therapy • Old method: high-dose monotherapy • Recent studies (ex. ALLHAT) • At least 2 medications of different classes to treat mild hypertension • 3 or 4 different medications to treat more difficult cases • Thiazide-type antihypertensive medications cost-effective • Initial treatment: • Beta blockers, Angiotensin-converting enzyme (ACE) inhibitors, Angiotensin receptor blockers, Calcium antagonists Cecil, 2004
Stage 2 Drug Therapy • JNC recommends: • 2 drug combination • Additional medications needed for each 10 mm Hg of systolic BP above goal • Great majority should include low-dose diuretic • High-risk conditions (heart failure/diabetes) • Angiotensin-converting enzyme inhibitors (ACE-Is) • Angiotensin receptor blockers (ARBs) Cecil, 2004
Cardio Events in Hypertensive Patients Verdecchia, Carin, Circo,2001
Left Ventricular Hypertrophy www.medem.com, 2007
Counseling Patients: Contradictions & Side Effects Considerations For Individualizing Antihypertensive Drug Therapy
Hypertensive Sub-Populations • Hypertensive patients with nephrosclerosis • Diabetic hypertensive patients • Hypertensive patients with coronary artery disease • Isolated systolic hypertension in older persons • Hypertensive disorders of women • Oral contraceptives • Pregnancy Cecil, 2004
Hypertension Case Study How would we modify his treatment since he did not change his health behaviors (and he is diabetic)?